Download
1 / 74
780 likes | 830 Views
Presentation throws some light on Masticatory muscles... and Disorders of masticatory muscle ...

E N D
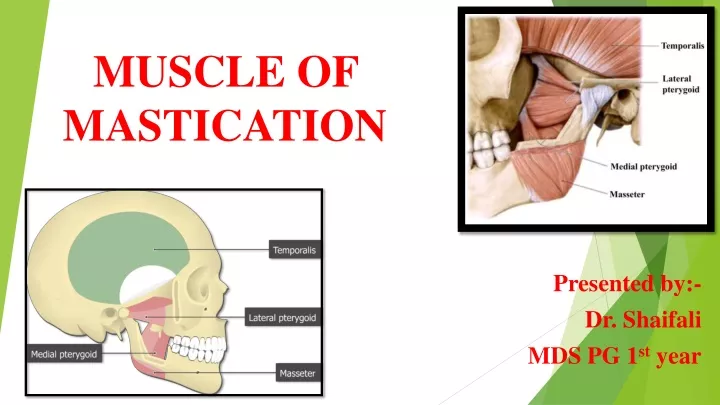
MUSCLE OF MASTICATION Presented by:- Dr. Shaifali MDS PG 1st year
CONTENTS:- • Introduction • Embryology of muscle of mastication • Types: Muscles of mastication (Primary and accessory) • Anatomy • Disorders of the Masticatory Muscle • Conclusion • References
INTRODUCTION MUSCLE: Muscle is a contractile tissue of the body and is derived from the mesodermal layer of embryonic germ cells. Muscle cells contain contractile filaments that move past each other and change the size of the cell. MUSCLE OF MASTICATION: The muscles of mastication move the mandible during mastication and speech.
EMBRYOLOGY OF MUSCLE OF MASTICATION • They develop from the mesoderm of the first branchial arch, and are supplied by the mandibular nerve which is the nerve of that arch. • Posterior belly of digastric muscle develops from second branchial arch and is supplied by facial nerve.
PRIMARY MUSCLE OF MASTICATION Masseter Temporalis Lateral pterygoid Medial pterygoid
Accessory Muscles Of Mastication • Buccinator • Suprahyoid muscles (Digastric muscle, Mylohyoid muscle, and Geniohyoid muscle)
MASSETER • Quadrilateral in shape. • Covers the lateral aspect of the ramus and the coronoid process of the mandible. • It has three layers : Superficial , Middle , and Deep
ORIGIN : • SUPERFICIAL LAYER (largest) : from anterior 2/3 of lower border of zygomatic arch and adjoining zygomatic process of maxilla. • MIDDLE LAYER : from anterior 2/3 of deep surface and posterior 1/3 of lower border of zygomatic arch. • DEEP LAYER : from deep surface of zygomatic arch.
INSERTION : • Superficial layer : into lower part of lateral surface of ramus of mandible. • Middle layer : into middle part of ramus. • Deep layer : into upper part of ramus and coronoid process of mandible.
FIBRES: • Superficial fibres pass downwards and backwards at 45 degrees • Middle and Deep fibres pass vertically downwards. • Three layers are separated posteroinferiorly by an artery and a nerve.
NERVE SUPPLY : Masseteric Nerve (A branch of anterior division of mandibular nerve) ACTIONS : Elevates mandible to close the mouth to bite.
TEMPORALIS • Fan shaped muscle. • Bipennate muscle. • Fills the temporal fossa. FIBRES: Converge and pass through gap deep to zygomatic arch.
TEMPORAL FASCIA: • The temporal fascia is a thick aponeurotic sheet that roofs over the temporal fossa and covers the temporalis muscle. • Superiorly, the fascia is single layered and is attached to the superior temporal line. Inferiorly, it splits into two layers which are attached to the inner and outer lips of the upper border of the zygomatic arch . • The deep surface of the temporal fascia gives origin to some fibres of the temporalis muscle.
ORIGIN: • Temporal fossa, excluding zygomatic bone. • Temporal Fascia. INSERTION: • Margins and deep surface of coronoid process • Anterior border of ramus of mandible.
NERVE SUPPLY : • Two deep temporal branches from anterior division of mandibular nerve.
ACTIONS: • Elevates mandible. • Posterior fibres retract the protruded mandible. • Helps in side to side grinding movement.
LATERAL PTERYGOID • Short, conical. • Has upper and lower heads.
ORIGIN: • Upper head (small) : originates from infratemporal surface and crest of greater wing of sphenoid bone. • Lower head (larger) : originates from lateral surface of lateral pterygoid plate.
INSERTION: • Pterygoid fovea on the anterior surface of neck of mandible. • Anterior margin of articular disc and capsule of TMJ. Insertion is posterolateral and at a slightly higher level than origin. FIBRES: Fibres run backwards and laterally and converge for insertion.
NERVE SUPPLY: • A branch from anterior division of mandibular nerve. ACTIONS: • Depress mandible to open mouth with suprahyoid muscles. • Lateral and medial pterygoid protrude mandible. • Left lateral pterygoid and right medial pterygoid turn the chin to left side as part of grinding movements.
VASCULAR SUPPLY • Pterygoid branch of 2nd part ofmaxillaryartery
MEDIAL PTERYGOID • Quadrilateral. • Has a small superficial and a large deep head.
ORIGIN: • Superficial Head (small slip) : from tuberosity of maxilla and adjoining bone. • Deep Head (quite large): from medial surface of lateral pterygoid plate and adjoining process of palatine bone. INSERTION: Roughened area on the medial surface of Angle & adjoining ramus of mandible, below & behind the mandibular foramen & mylohyoid groove.
FIBRES: Fibres run downwards, backwards and laterally.
NERVE SUPPLY: • Nerve to medial pterygoid, branch of the main trunk of mandibular nerve.
VASCULAR SUPPLY Pterygoid branch of 2nd part ofmaxillary artery
ACTIONS: • Elevates mandible. • Helps protrude mandible. • Right medial pterygoid with left lateral pterygoid turn the chin to left side.
Accessory Muscles Of Mastication BUCCINATOR • Is thin quadrilateral facial muscle. ORIGIN: • Upper fibres, from maxilla opposite molar teeth. • Lower fibres, from mandible, opposite molar teeth. • Middle fibres, from pterygomandibular raphae
INSERTION: • Upper fibres, straight to the upper lip. • Lower fibres, straight to the lower lip. • Middle fibres decussate before passing to the lips. ACTION: • Flattens cheek against gums and teeth; prevents accumulation of food in the vestibule. • This is the whistling muscle.
DIGASTRIC MUSCLE • Suprahyoid muscle. • Has two bellies united by an intermediate tendon.
ORIGIN: • Anterior belly (DGA) : from digastric fossa of mandible. • Posterior belly (DGA) : from mastoid notch of temporal bone. INSERTION: Both ends meet at the intermediate tendon which perforates stylohyoid and is held by a fibrous pulley to the hyoid bone.
FIBRES: • Anterior belly runs downwards and backwards. • Posterior belly runs downwards and forwards. NERVE SUPPLY: • Anterior belly by nerve to mylohyoid. • Posterior belly by facial nerve.
ACTIONS: • Depresses mandible when mouth is opened widely or against resistance; it is secondary to lateral pterygoid. • Elevates hyoid bone.
MYLOHYOID • Flattriangular • Two mylohyoids form floor of the oralcavity.
ORIGIN: • Mylohyoid line ofmandible. INSERTION: • Posterior fibers : body of the hyoidbone. • Middle and anterior fibers : medianraphae, between mandible and hyoid bone.
FIBRES: • Runs medially and slightly downwards. NERVE SUPPLY: Mylohyoid Nerve . ACTIONS: • Elevates floor of mouth in first stage of deglutition. • Helps in depression of mandible, and elevation of hyoid bone.
GENIOHYOID • Short and narrow muscle, lies above medial part ofmylohyoid. ORIGIN: Inferior mental spine (genial tubercle) INSERTION: Anterior surface of body of hyoid bone.
FIBRES: • Runs backwards and downwards. ACTIONS: • Elevates hyoid bone • May depress mandible when hyoid is fixed.
Disorders of the Masticatory Muscle • Masticatory muscle disorders are a group of musculoskeletal conditions that are the major cause of nonodontogenic pain in the orofacial region. • There are several types of disorders of the masticatory muscles, each of which may have a complex etiology, clinical course, and response to therapy. • Mechanisms behind masticatory muscle pain include overuse of a normally perfused muscle or ischemia of a normally working muscle, sympathetic reflexes that produce changes in vascular supply and muscle tone, and changes in psychological and emotional states.
MUSCLE HYPERTROPHY • Hypertrophy refers to an enlargement caused by an increase in the size, but not in the number of cells. • Generalized masticatory muscle hypertrophy may affect the temporalis, masseter, and medial pterygoid muscles in a variety ofcombination. • Masseter muscle hypertrophy in itself has been postulated to be associated with awake and sleep bruxism as a possible result of prolonged tooth clenching (Manfredini et al. 2013a; Castroflorio et al. 2015b). • Masseteric hypertrophy may present as either unilateral or bilateral painless swelling of unknown origin in the region of angle of mandible.
MUSCLE HYPERPLASIA • Muscle hyperplasia results in an increase in the number of fibers within a muscle. • However masticatory muscle hyperplasia is very rare, with the exception of the Masticatory muscle tendon-aponeurosis hyperplasia (MMTAH) (Sato and Yoda 2016). • MMTAH is a condition in which the tendon and aponeurosis of the bilateral masticatory muscles exhibit hyperplasia, thus restricting muscle extension.
Etiology -- still remains unclear, although parafunctional habits are often associated with it. A hard cord-like structure found along the anterior border of the masseter muscle on intraoral palpation can help in clinical diagnosis, although MRI can help visualize tendons and aponeuroses. • Symptom -- limited mouth opening. • The definitive diagnosis between masticatory muscle hypertrophy and masticatory muscle hyperplasia can only be established by histology. • Treatment -- Aponeurectomy combined with coronoidectomy is the treatment of choice for a better prognosis.
MYALGIA • According to DC/TMD, masticatory muscle pain or myalgia can be defined as a pain of muscle origin that is affected by jaw movement, function, or parafunction, and replication of this pain occurs with provocation testing of the masticatory muscles. Features of Local Myalgia • Sore MOM with pain in cheeks and temples on chewing, wide opening, and often on waking (eg. nocturnal bruxism) , • Bilateral, • Described as stiff, sore, aching, spasm, tightness, or cramping, • Sensation of muscle stiffness, weakness, fatigue , • Possible reduced mandibular range of motion .
Myalgia is further subdivided into three mutually exclusive subtypes :
Myofascial pain syndrome (MPS) • Myofascial pain syndrome (MPS) is described as the sensory, motor, and autonomic symptoms caused by myofascial Trigger points. The best available evidence supports that TrPs develop after muscle overuse. • Myofascial TrPs, are described as hyperirritable spots in the fascia surrounding skeletal muscle.
Unexplained pain frequently radiates from these points of local tenderness to broader areas, sometimes distant from the TrP itself. • The treatment of MPS focuses on analgesics and anti-inflammatory therapy, followed by: Physiotherapy, Occlusal splint therapy, Laser therapy, Transcutaneous electric nerve stimulation (TENS), Acupuncture, and Biofeedback (Pal et al. 2014).
MYOSITIS • Myositis is a primary inflammation of muscle resulting from infection such as viruses, including the common cold, flu, and human immunodeficiency virus (HIV) or trauma. • It is characterized by constant acute pain and is usually accompanied by swelling, redness of the overlying skin, and increased temperature over the affected muscle (Greene and Laskin 2013). • Myositis can be differentiated from other forms of myalgia by its acute presentation and constant nature of the reported pain, its associated sequelae such as the patient’s acute and unambiguous responses to muscle palpation, and a history of recent trauma or infection (Lundberg and Vencovsky 2017).