Download
1 / 9
90 likes | 93 Views
Malaria is an acute febrile illness caused by Plasmodium parasites, which are spread to people through the bites of infected female Anopheles mosquitoes. There are 5 parasite species that cause malaria in humans, and 2 of these species u2013 P. falciparum and P. vivax u2013 pose the greatest threat. P. falciparum is the deadliest malaria parasite and the most prevalent on the African continent. P. vivax is the dominant malaria parasite in most countries outside of sub-Saharan Africa.

E N D
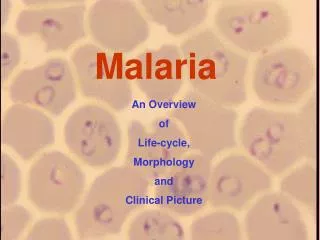
MalariaDefinition: infection with protozoa, plasmodium vivax, P. ovale, P. malaria, or P. falciparum. View slides
Usually, people get malaria by being bitten by an infective female Anopheles mosquito. Only Anopheles mosquitoes can transmit malaria and they must have been infected through a previous blood meal taken from an infected person.
Plasmodium life cycle1.Sporozoites injected through human skin by female anopheline mosquito, then migrate to liver.2. In the hepatocytes, they multiply into merozoites. After 1-4 weeks incubation, the hepatocytes rupture and the merozoites are released into the blood. P. vivax and P. ovale can also become hypnozoites, incubating in liver for months or even years.3. Enter RBCs and become trophozoites then schizonts, which form further merozoites, leading to rupture and hence hemolysis and fever in 48-72 hr cycles. Some merozoites become gametocytes, which are taken up in RBCs by mosquitoes feeding on blood.4. P. falciparum is the most pathogenic as it affects all RBC ages, including reticulocytes, while others only affect mature RBCs.
Signs and symptomsGeneral:1. Fever: all tertian (48-hourly) except quartan (72-hourly) in P. malaria. These classic patterns aren't always clearly seen.2. Rigors3. Headache4. Diarrhea and vomiting.5. HepatosplenomegalyFalciparum malaria:1. Flu-like prodrome: myalgia, malaise, headache, anorexia.2. Irregular fever initially.3. JaundiceComplicated falciparum malaria:1. Mortality approaches 100% if severe and untreated.2. Cerebral malaria: altered mental status, seizures, coma, decerebrate posturing, ↑plantars, teeth-grinding.3. AKI4. Bleeding: hemoglobinuria ('blackwater fever'), DIC, retinal hemorrhages.5. Metabolic: ↓glucose, metabolic acidosis, Kussmaul's breathing.6. ARDS and pulmonary oedema.7. Splenic rupture.8. Shock
InvestigationsDiagnosis using blood films:1. Serial testing: up to 3 times if 1st -ve.2. Thick film – quick yes or no malaria – and thin film – which subtype.3. Also shows parasitemia (%RBCs infected) and stage, with imminent decline in patient condition due if there are ↑schizonts. Dangerous if parasitemia >2% and life-threatening if >5%.4. Simple but less sensitive antigen detection kits are available too.Bloods:1. FBC: anemia, ↓platelets. Low platelets result from increased splenic activity during hemolysis, leading to excess platelet clearance.2. Coag: DIC.3. ↓Glucose4. ABG: metabolic acidosis. U+E: AKI.Other tests:1. Urinalysis: blood.2. Blood cultures to rule out bacterial sepsis.
ManagementProphylaxisStart 1 week before to check for side effects, and continue until 4 weeks after.Areas without chloroquine resistant falciparum:1. Chloroquine (daily) plus proguanil (weekly). Areas with chloroquine resistance. Any 1 of:1. Atovaquone/proguanil (Malarone). Few side effects, and is taken from 1 day before until 7 days afterwards. Expensive. 2. Doxycycline 3. Mefloquine (Lariam): once weekly. Also:1. Long sleeves dusk till dawn. 2. Mosquito nets 3. DEET repellent.
Treatment1.P. vivax, P. ovale, and P. malaria: chloroquine plus primaquine.2. Uncomplicated P. falciparum: 1st-line artemether/lumefantrine (Riamet). 2nd-line: quinine/doxycycline (quinine/clindamycin in kids), or atovaquone/proguanil.3. Complicated P. falciparum (cerebral, renal, or shock): artesunate IV (preferably), or quinine IV + doxycycline IV/PO. Careful monitoring of fluid, lactate, U+E. Transfuse if anemic.
Complications1.P. vivax and P. ovale can remain dormant in the liver as hypnozoites and relapse years later. Causes tropical splenomegaly syndrome if recurrent.2. P. malaria can lie low in blood for years, with or without symptoms.For more information,you can visit our website : medicospdf.com you can also find us on google and apple store. Search Medicos PDF thank you.This slides is made by Medicos team, please keep supporting medicos team. Thank you.