Download
1 / 41
420 likes | 1.03k Views
Cutaneous Anthrax. View Table. Mimics: Ecthyma Brown Recluse Spider Bite Acute Febrile Neutrophilic Dermatosis (Sweet's Syndrome) Folliculitis, Furuncle, Carbuncle, & Cutaneous Abscess Pyoderma Gangrenosum Orf Virus Infection . Variola (Smallpox). View Table. Mimics:

E N D
Cutaneous Anthrax View Table • Mimics: • Ecthyma • Brown Recluse Spider Bite • Acute Febrile Neutrophilic Dermatosis (Sweet's Syndrome) • Folliculitis, Furuncle, Carbuncle, & Cutaneous Abscess • Pyoderma Gangrenosum • Orf Virus Infection Variola (Smallpox) View Table • Mimics: • Varicella (Chickenpox) • Herpes Zoster (Shingles) • Molluscum Contagiosum
Cutaneous Anthrax Back
Variola (Smallpox) Back
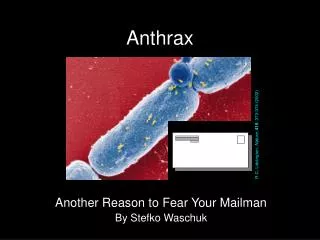
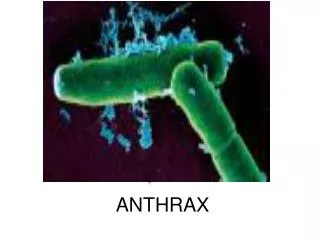
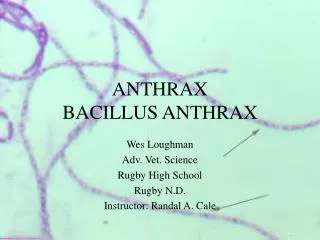
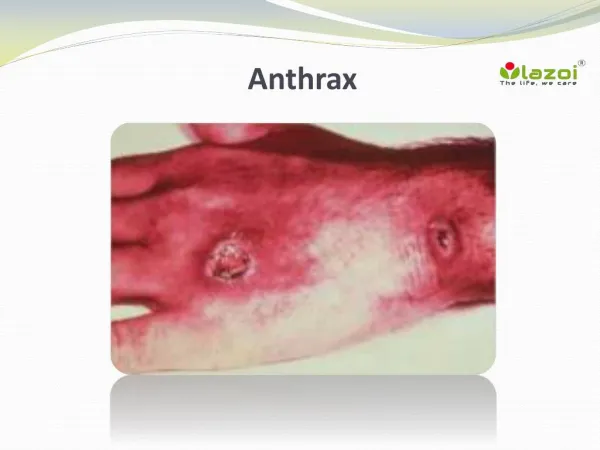
Cutaneous Anthrax View Table The primary lesion of cutaneous anthrax is a painless, pruritic papule that appears one to seven days after inoculation. Within one to two days, small vesicles or a larger, 1- to 2-cm vesicle forms that is filled with clear or serosanguineous fluid. As the vesicle enlarges, satellite vesicles may form. Fitzpatrick’s Dermatology in General Medicine. Fifth Edition. Freedberk IM, Eizen, AZ, Wolff, K, Austen KF, Goldsmith LA, Katz SI, Fitzpatrick TB (eds.). New York: The McGraw Hill Companies, Inc; 1999. Fluid within the vesicles may contain numerous, large gram-positive bacilli. As the lesion matures, a prominent, non-pitting edema surrounds it. Eventually, the vesicle ruptures, undergoes necrosis, and enlarges, forming an ulcer covered by the characteristic black eschar. Symptoms include low-grade fever and malaise. Regional lymphadenopathy is present early on.
Ecthyma View Table
Ecthyma View Table Ecthyma is a condition in which the exudate or crust of a pyogenic infection involves the entire epidermis. The crust can be thick and adherent. Ecthyma is usually the consequence of neglected impetigo caused by Staphylococcus aureus or group A streptococcus. Ecthymatous lesions can evolve from localized skin abscesses (boils) or within sites of preexisting trauma. The margin of the ecthyma ulcer can be indurated, raised, and violaceous. Untreated ecthymatous lesions can enlarge over the course of weeks or months to a diameter of 2 to 3 cm. Staphylococcal and streptococcal ecthyma occurs most commonly on the lower extremities of children, the elderly, and people who have diabetes. Poor hygiene and neglect are key elements in its pathogenesis. Ecthyma gangrenosum is a cutaneous ulcer caused by Pseudomonas aeruginosa; it resembles ecthyma caused by staphylococcal or streptococcal organisms. Ecthyma gangrenosum, which usually occurs in individuals with prolonged neutropenia, can be associated with Pseudomonas bacteremia.
Differential Dx - Ecthyma View Table • Cutaneous anthrax • Lesion located most commonly on upper extremities (especially the hands), neck, or face • Systemic manifestations include fever, malaise, regional lymphadenopathy • Ecthyma • Lesions located most commonly on lower extremities • Systemic symptoms unusual • Ecthymagangrenosum • Associated with neutropenia • May be associated with Pseudomonas bacteremia
Brown Recluse Spider Bite View Table
Brown Recluse Spider Bite View Table • The brown recluse spider, Loxosceles reclusa: • is widely distributed in the U.S. throughout the Southeast and Midwest • natural habitat is outdoors under overhanging rocks and cliffs • lives in closets, attics, and outbuildings • hibernates during the winter, so most bites occur between March and October • Responses to bites range from mild local urticarial (hive-like) reactions to full-thickness skin necrosis. The more extensive reactions may be associated with systemic manifestations including a maculopapular rash, fever, headache, malaise, joint aches, and nausea and vomiting. • The bite itself is generally painless, and the findings of a central papule and associated redness may not be seen for 6 to 12 hours.
Brown Recluse Spider Bite View Table Only approximately 10% of bites progress to skin necrosis; those that do tend to show progression in 48 to 72 hours. Central blistering with a surrounding gray to purple discoloration at the bite site may appear. The site is surrounded by a ring of blanched skin that in turn is surrounded by a large area of redness, producing the "red, white, and blue" sign typical of a brown recluse spider bite. At this stage, the bite is associated with significant pain. As the wound becomes necrotic, it will turn black. Healing is slow and may require skin grafting to cover the defect. Not all victims recall the spider bite, and because the clinical appearance is nonspecific, diagnosis can be difficult.
Differential Dx – Brown Recluse View Table • Cutaneous anthrax • Painless lesion • Necrosis of skin and subcutaneous tissue occurs late and gradually • Brown Recluse Spider Bite • Bite lesion becomes painful • Necrosis of skin and subcutaneous tissue occurs early and quickly
Acute Febrile Neutrophilic Dermatosis (Sweet's Syndrome) View Table
Acute Febrile Neutrophilic Dermatosis (Sweet's Syndrome) View Table Acute febrile neutrophilic dermatosis, or Sweet's syndrome, is characterized by the presence of recurrent, painful, plaque-forming inflammatory papules, and sometimes fever and systemic leukocytosis. There is no known cause of Sweet's syndrome. Approximately 20 percent of cases are associated with malignancy. The typical skin lesions are red or bluish-red papules or nodules that tend to coalesce to form irregular, sharply demarcated plaques. There is an associated inflammatory edema within the lesion that gives the illusion of vesicles on the surface of the lesion. In later stages, the tops of the papules may become studded with tiny pustules.
Acute Febrile Neutrophilic Dermatosis (Sweet's Syndrome) View Table The lesions of Sweet's syndrome are tender and often painful, and are likely to enlarge over a period of days to weeks. The presentation can be a single lesion or multiple lesions. The eruption occurs characteristically on the upper extremities, face, or neck, but it can also develop on the lower extremities. Systemic symptoms can include fever and leukocytosis; patients can appear very ill. Not all patients express the entire spectrum of findings, however, and fever and leukocytosis may be absent. Other symptoms may include headache, joint pain, myalgias, and malaise.
Differential Dx – Sweet’s View Table • Cutaneous anthrax • Solitary lesion • Painless lesion • Necrotic ulceration • Formation of black eschar • Characteristic massive edema surrounds the lesion • Sweet’s Syndrome • Multiple lesions most common • Painful or tender lesions • Edema within the lesions
Folliculitis, Furuncle, Carbuncle, and Cutaneous Abscess View Table Carbuncle on the back of the neck. Notice the elevated red lesion with multiple draining pustules.
Folliculitis, Furuncle, Carbuncle, and Cutaneous Abscess View Table Folliculitis is characterized by the formation of a circumscribed, conical pustule around a hair follicle. A furuncle is a deep, necrotizing form of folliculitis, with pus accumulation. Several furuncles may coalesce to form a carbuncle. An abscess (boil) is a localized accumulation of purulent material deep in the dermis or subcutaneous tissue. Pus may not be visible on the surface of the skin. An abscess is warm, red, and tender; it frequently begins as folliculitis. Most furuncles and carbuncles are caused by Staphylococcus aureus. Fever and malaise sometimes accompany carbuncles and abscesses.
Folliculitis, Furuncle, Carbuncle, and Cutaneous Abscess View Table A furuncle starts as a hard, tender, red nodule in hair-bearing skin that enlarges and becomes painful and fluctuant. Rupture may occur with drainage of pus. The pain then subsides, and the redness and swelling subside over several days or weeks. A carbuncle is larger than a furuncle, typically occurring at the nape of the neck or on the back or thighs. The lesion is red, indurated, painful, and multiple pustules soon appear on its surface, draining around multiple hair follicles. The lesion develops a yellow-gray crater at the center and heals slowly by granulation.
Differential Dx – Folliculitis View Table • Cutaneous anthrax • Painless lesion • Lesion does not drain pus, is not necessarily associated with hair follicle • Vesicle ulcerates and forms characteristic black eschar • Furuncles, carbuncles, and abscesses • Painful lesion • Pus-draining lesion surrounding hair follicle
Pyoderma Gangrenosum View Table
Pyoderma Gangrenosum View Table Pyoderma gangrenosum is a destructive, inflammatory skin disease in which a painful nodule or pustule breaks down to form a progressively enlarging ulcer, with a raised, tender, undermined border. Pyoderma gangrenosum can sometimes occur in the presence of an underlying systemic disorder such as ulcerative colitis, Crohn's disease, arthritis, gammopathy, or other conditions. The distinguishing feature of pyoderma gangrenosum is an ulcer with a raised, inflammatory border and a boggy, necrotic base. It starts as a deep, painful nodule, or as a superficial hemorrhagic pustule. The lesion breaks down and ulcerates, discharging a purulent, hemorrhagic exudate.
Pyoderma Gangrenosum View Table The border is irregular, elevated, and dusky-red or purplish. A halo of bright erythema surrounds the margin of an advancing ulcer. The base of the ulcer is usually covered with necrotic material and studded with small abscesses. Lesions are often solitary, but may arise in clusters and can involve any area of the body. The onset of pyoderma can be explosive, characterized by pain, toxicity, and fever, or indolent and slow with massive granulation within the ulcer, as well as crusting. Almost invariably, the lesions are painful.
Differential Dx – Pyoderma Gangrenosum View Table • Cutaneous anthrax • Painless lesion • Lesion associated with characteristic edema • Forms an eschar • Pyoderma Gangrenosum • Painful lesion • Purulent lesion
Orf Virus Infection View Table Orf virus is a member of the Poxviridae family. It produces disease mainly among sheep, goats, and musk oxen, but it can be transmitted to humans. Farmers and veterinarians are among the most likely to be exposed to the virus. The orf lesion is approximately 1.5 cm in diameter, and is usually a solitary lesion located on the dorsal aspect of the finger. Regional lymphadenopathy, lymphangitis, and fever are common symptoms. The disease passes through several distinct stages: • The lesion begins as a red, solid, elevated papule. • It enlarges into a nodule with a red center, white middle ring, and red periphery (the target stage). • In the acute stage, a red weeping surface is present. • In the regenerative stage, a thin, dry crust develops, through which black dots may be seen covering the surface of the nodule. • Small papillomas, or tiny growths, cover the surface. • During the regressive phase, a thick crust develops over the surface of the lesion, papillomas decrease in size, and the lesion flattens out.
Differential Dx – Orf Virus View Table • Cutaneous anthrax • Lesion forms black eschar surrounded by massive edema • Orf Virus Infection • Lesion forms crusts, scabbing
Variola (Smallpox) View Table Smallpox in a man: Notice the diffuse and extensive distribution of lesions.
Variola (Smallpox) View Table Smallpox in a child: Notice that all lesions are in the same stage of development.
Variola (Smallpox) View Table • Smallpox is an acute exanthematous disease caused by infection with the poxvirus variola. • The significant clinical features include: • Three-day prodromal illness characterized by fever, headache, backache, and vomiting. • Generalized centrifugal rash that follows • Begins centrally then spreads to the extremities • Rapid succession of papules, vesicles, pustules, umbilication, and crusting over a 14-day period. • Prior vaccination may alter the clinical presentation of smallpox. The following description applies to the classic presentation in unvaccinated individuals.
Variola (Smallpox) View Table A macular red rash may precede the appearance of the papules, which are tense to palpation. Papules soon vesiculate, forming a circumscribed, elevated lesion that contains clear fluid. The rash at this point can be very sparse, although individual vesicles can coalesce to form large patches. As the vesicles mature, they turn into pustules. Central umbilication of the pustule is characteristic of smallpox. Eventually, the pustule crusts over and heals with scar formation. A second important distinguishing characteristic of smallpox is that all of the lesions at a given time are in the same stage of development. That is, at any one point in time the lesions are all papules or vesicles or pustules. Bacterial infection of the lesions can occur, producing localized abscesses and cellulitis.
Varicella (Chickenpox) View Table Chickenpox vesicle behind the ear. Notice the translucent quality of the vesicle on the skin, the classic "dew drop on a rose petal" appearance. Chickenpox on the palate. Notice the glistening, water-drop characteristic of the chickenpox vesicle on the palate.
Varicella (Chickenpox) View Table Chickenpox on the hand. Notice the simultaneous occurrence of lesions in different stages of development. Chickenpox in an infant. Notice the rose-colored macules, papules, vesicles, pustules, necrotic pustules, and crusted lesions occurring simultaneously.
Varicella (Chickenpox) View Table Varicella (chickenpox) and herpes zoster (shingles) are distinct clinical entities cause by the varicella-zoster virus (VZV). In young children, prodromal symptoms of chickenpox are uncommon, but in older children and adults, the manifestation of the rash may be preceded by two or three days of fever and chills, malaise, headache, backache, sore throat, and dry cough. The rash begins on the face and scalp and spreads rapidly to the trunk, with relative sparing of the extremities. New lesions arise in crops, usually appearing centrally. Each crop proceeds through the developmental phase described below, so that at any given time, a patient can have macules, papules, vesicles, pustules, and crusts. In smallpox, by contrast, at any given time, all lesions on the patient's body are in the same phase of development.
Varicella (Chickenpox) View Table The first sign of chickenpox is rose-colored macules that rapidly progress to papules then to vesicles, then to pustules, and finally to scabbing over with crusts. The typical wall of the vesicle is so thin that it often resembles a drop of water on the reddened surface of the skin (the "dew drop on a rose petal" appearance). As the lesion dries and changes from a vesicle to a pustule, it umbilicates and then crusts over. The crusts fall off in one to two weeks. Scarring is rare unless the lesions become secondarily infected vesicles can occur on the mucous membranes, most commonly on the palate; they can also occur in the nose, pharynx, larynx, trachea, gastrointestinal tract, conjunctiva, and vagina.
Differential Dx - Chickenpox View Table Chickenpox • Begins on the face and scalp, spreads to the trunk • Lesions in various stages of development can simultaneously be present on the patient's skin Variola (Smallpox) • Begins centrally, then spreads outward to face and extremities • All lesions are always in a single stage of development
Herpes Zoster (Shingles) View Table Herpes (varicella) zoster on the arm. Notice the characteristic grouping of vesicles Varicella zoster on the face. Notice the dermatomal distribution of the papules, vesicles, and pustules.
Herpes Zoster (Shingles) View Table Herpes zoster is a localized disease caused by the varicella-zoster virus (VZV). It is characterized by unilateral radicular pain and a vesicular eruption that is typically limited to one or two dermatomes innervated by a spinal or cranial nerve. The most distinctive characteristics of herpes zoster are its localization and it distribution, which is almost always unilateral. The individual lesions of varicella (chickenpox) and of zoster are identical, but the lesions of zoster evolve more slowly and are characterized by grouped vesicles. The lesions of varicella, by contrast, are more widely distributed. As in varicella, zoster vesicles evolve into pustules, then dry and crust.
Differential Dx – Herpes Zoster View Table Herpes Zoster (Shingles) • Lesions are unilaterally distributed along a dermatome • Lesions at any given time are in different stages of development (vesicles, pustules, and crusts are in evidence at one time) Variola (Smallpox) • Lesions are widely distributed • Lesions at any given time are all at the same stage of development • Associated with severe constitutional symptoms
Molluscum Contagiosum View Table Molluscum contagiosum is a common, benign viral infection of the skin and mucous membranes caused by the molluscum contagiosum virus. It typically affects children, but can be transmitted sexually in adults. The mature lesion is an umbilicated papule.
Molluscum Contagiosum View Table Lesions begin as small (3 to 6 mm) papules that are smooth, flesh-colored domes with a central dimple. Inside the papule is a white, curd-like core that can be easily expressed. Lesions can occur anywhere on the skin and mucous membranes, but are usually grouped in one or two areas. Occasionally, they may be widely disseminated. Typically fewer than 20 lesions are present, but some individuals may have hundreds. The head, eyelids, trunk, and genitalia are most commonly affected, the genitalia being the predominant site in adults. The lesions are characteristically asymptomatic, but a few patients may complain of itching or may develop an eczematous reaction around the lesions.
Differential Dx – Molluscum Contagiosum View Table Molluscum Contagiosum • Lesions usually grouped in one or two areas • Not associated with clinical symptoms • Lesions are papules only Variola (Smallpox) • Lesions are widespread • Associated with severe clinical symptoms • Lesions progress from macules to vesicles to papules to crusts (progression occurs all at the same time in smallpox but at different times in chickenpox)
For the latest information on diagnosis and treatment of the diseases and conditions of bioterrorism, visit the Bioterrorism Resource Center on ACPOnline at: http://www.acponline.org/bioterro/