Download
1 / 14
140 likes | 786 Views
Presentation on Cardiogenic Shock for nursing students.

E N D
An IntroductionCardiogenic shock Medical & Surgical Nursing For Nursing Students Prepared By: Deepak Kapoor (kapoor.deepak@live.com)
Introduction Cardiogenic (kar-dee-oh-JE-nik) shock is a state in which a weakened heart isn't able to pump enough blood to meet the body's needs. It is a medical emergency and is fatal if not treated right away. The most common cause of cardiogenic shock is damage to the heart muscle from a severe heart attack. Not everyone who has a heart attack develops cardiogenic shock. In fact, less than 10 percent of people who have a heart attack develop it. But when cardiogenic shock does occur, it's very dangerous. For people who die from a heart attack in a hospital, cardiogenic shock is the most common cause. Definition Cardiogenic shock resulting from failure of the heart to pump an adequate amount of blood as a result of heart disease and especially heart attack.
MI is the most common cause of cardiogenic shock in modern times. Morgagni first recognized MI in 1761, and it was subsequently described by Caleb Parry in 1788 and by Heberden in 1802. John Hunter, a surgeon at St. George's Hospital in London, England described his personal experience with MI in 1773. Adam Hammer, a physician in Mannheim, Germany, identified the role of coronary thrombosis in the causation of MI in 1878. The clinical features of acute MI and survival of patients after such an event were reported in 1912 in the Journal of the American Medical Association by James Herrick, a Chicago physician. In the late 20th century, clinicians recognized cardiogenic shock as a low cardiac output state secondary to extensive left ventricular infarction, development of a mechanical defect (eg, ventricular septal defect or papillary muscle rupture), and right ventricular (RV) infarction. Historical aspects Giovanni Battista Morgagni (1682-1771) MI is the most common cause of cardiogenic shock in modern times. Morgagni first recognized MI in 1761, and it was subsequently described by Caleb Parry in 1788 and by Heberden in 1802. John Hunter, a surgeon at St. George's Hospital in London, England described his personal experience with MI in 1773. Adam Hammer, a physician in Mannheim, Germany, identified the role of coronary thrombosis in the causation of MI in 1878. The clinical features of acute MI and survival of patients after such an event were reported in 1912 in the Journal of the American Medical Association by James Herrick, a Chicago physician. In the late 20th century, clinicians recognized cardiogenic shock as a low cardiac output state secondary to extensive left ventricular infarction, development of a mechanical defect (eg, ventricular septal defect or papillary muscle rupture), and right ventricular (RV) infarction. Caleb Hillier Parry (1755–1822)
Incidence mortality remains over 50% in most studies 5-10% of patients who suffer a myocardial infarction Cardiogenic shock continues to occur in 5-10% of patients who suffer a myocardial infarction and the mortality remains over 50% in most studies.
Etiology • A large section of heart muscle that no longer moves well or does not move at all • Breaking open (rupture) of the heart muscle due to damage from the heart attack • Dangerous heart rhythms, such as ventricular tachycardia, ventricular fibrillation, or supraventricular tachycardia • Tear or rupture of the muscles or tendons that support the heart valves, especially the mitral valve • Tear or rupture of the wall (septum) between the left and right ventricles (lower heart chambers) • Very slow heart rhythm (bradycardia) or problem with the electrical system of the heart (heart block) Shock occurs whenever the heart is unable to pump as much blood as the body needs. The most common causes are serious heart complications. Many of these occur during or after a heart attack (myocardial infarction). These complications include:
Clinical Manifestation Chest pain or pressure Fast breathing Fast pulse Heavy sweating, moist skin Restlessness, agitation, confusion Shortness of breath Skin that feels cool to the touch Pale skin color or blotchy skin Weak (thready) pulse Decreased mental ability Loss of ability to concentrate Loss of alertness Coma (loss of consciousness)
Diagnosis An examination will show: Low blood pressure (usually less than 90 systolic) Blood pressure drop of more than 10 points when you stand up after lying down (orthostatic hypotension) Weak (thready) pulse To diagnose cardiogenic shock, a catheter (tube) may be placed in the lung artery (right heart catheterization). Tests may show that blood is backing up into the lungs and the heart is not pumping properly. Tests include: Cardiac catheterization Chest x-ray Coronary angiography Echocardiogram Electrocardiogram Nuclear scans
Diagnosis Other studies may be done to find out why the heart is not working properly. Lab tests include: Arterial blood gas Blood chemistry (chem-7, chem-20, electrolytes) Cardiac enzymes (troponin, CKMB) Complete blood count (CBC)
Medical Management Cardiogenic shock is a medical emergency. Patient will need to stay in the hospital, usually in the Intensive Care Unit. The goal of treatment is to find and treat the cause of shock to save patient’s life. Patient may need medicines to increase blood pressure and improve heart function, including: Dobutamine Dopamine Epinephrine Norepinephrine # These medicines may help in the short-term, but they should not be used over the long-term.
Medical Management When a heart rhythm disturbance (dysrhythmia) is serious, urgent treatment may be needed to restore a normal heart rhythm. This may include: Electrical "shock" therapy (defibrillation or cardioversion) Implanting a temporary pacemaker Medications given through a vein (intravenous) Patient may receive pain medicine if needed. Bed rest is recommended to reduce demands on the heart. Getting oxygen by a nasal tube or mask worn over the mouth lowers the workload of the heart helping the tissue of the body need less blood. Patient may receive intravenous fluids, including blood and blood products, if needed.
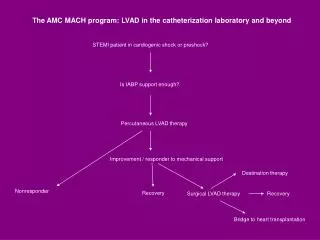
Surgical Management Other treatments for shock may include: Cardiac catheterization with coronary angioplasty and stenting Heart surgery (coronary artery bypass surgery, heart valve replacement, left ventricular assist device) Intra-aortic balloon counter pulsation (IABP) to improve heart and blood vessel function Pacemaker
Prognosis & Complications Prognosis In the past, the death rate from cardiogenic shock ranged from 80 - 90%. In more recent studies, this rate has decreased to 50 - 75%. When cardiogenic shock is not treated, the outlook is poor. Complications Brain damage Kidney damage Liver damage
Terminologies Ventricular tachycardia is a pulse rate of more than 100 beats per minute, with at least three irregular heartbeats in a row. Ventricular tachycardia (VT) is a rapid heartbeat that starts in the ventricles. Ventricular fibrillation (VF) is a severely abnormal heart rhythm (arrhythmia) that can be life-threatening. Paroxysmal supraventricular tachycardia (PSVT) is an occasional rapid heart rate. "Paroxysmal" means from time to time.
Thanks for Watching my presentation If you found my presentation useful, then please Join my group “Redefining The Nursing With New Outlook” over Facebook and contribute your ideas to make nursing profession on the heights. From: Deepak Kapoor (kapoor.deepak@live.com) Click here to find us