Download

1 / 12
0 likes | 7 Views
Triglyceride;<br>High-density<br>lipoprotein<br>cholesterol;<br>Ratio;<br>Cardiovascular<br>disease;

E N D
Nutrition, Metabolism & Cardiovascular Diseases (2022) 32, 318e329 Available online at www.sciencedirect.com Nutrition, Metabolism & Cardiovascular Diseases journal homepage: www.elsevier.com/locate/nmcd SYSTEMATIC REVIEWS AND META-ANALYSES Triglyceride to high-density lipoprotein cholesterol ratio and cardiovascular events in the general population: A systematic review and meta-analysis of cohort studies Yuxiong Chen1, Zhen’ge Chang1, Yijie Liu, Yakun Zhao, Jia Fu, Yongqiao Zhang, Yanbo Liu, Zhongjie Fan* Department of Cardiology, Peking Union Medical College Hospital, Peking Union Medical College & Chinese Academy of Medical Sciences, No. 1 Shuaifuyuan Wangfujing Dongcheng District, Beijing 100730, China Received 25 June 2021; received in revised form 20 October 2021; accepted 11 November 2021 Handling Editor: D. Noto Available online 18 November 2021 KEYWORDS Triglyceride; High-density lipoprotein cholesterol; Ratio; Cardiovascular disease; Meta-analysis Abstract has been regarded as a novel surrogate indicator of insulin resistance and the atherogenic index of plasma. This meta-analysis aimed to evaluate the association between the TG/HDL-C ratio and the incidence of cardiovascular events in the general population. Data synthesis: Cohort studies reporting the association between the TG/HDL-C ratio and cardio- vascular events in the general population were obtained by a systematic literature search of PubMed, Embase and Web of Science databases until April 11, 2021.13 cohort studies with a total of 207,515 participants were included in this meta-analysis. In a random-effects model, compared with those with the lowest category of the TG/HDL-C ratio, participants with the high- est category were independently associated with a higher risk of cardiovascular events (pooled HR: 1.43, 95%CI: 1.26e1.62, I2Z 72.9%). For the presence of publication bias detected by the Eg- ger’s test (p Z 0.011), correction for publication bias using the trim-and-fill method reduced the HR to 1.26 (95%CI: 1.11e1.44). This result was consistent with the finding of the TG/HDL-C ratio analyzed as a continuous variable (pooled HR per unit increment of the TG/HDL-C ratio: 1.08, 95% CI: 1.04e1.12, I2Z 67.0%). Subgroup analyses indicated that population gender, geographical re- gion, duration of follow-up, adjustment for other lipid parameters, adjustment for diabetes and categorical number did not significantly vary the relationship. Conclusion: Elevated TG/HDL-C ratio may be independently associated with an increased risk of cardiovascular events in the general population. More well-designed studies are needed to confirm the current findings. Registration number in PROSPERO: CRD42021244583. ª 2021 The Italian Diabetes Society, the Italian Society for the Study of Atherosclerosis, the Italian Society of Human Nutrition and the Department of Clinical Medicine and Surgery, Federico II University. Published by Elsevier B.V. All rights reserved. Aims: The ratio of triglyceride (TG) to high-density lipoprotein cholesterol (HDL-C) Abbreviations: CHD, Coronary heart disease; CI, Confidence interval; CVD, Cardiovascular diseases; HDL-C, High-density lipoprotein cholesterol; HR, Hazard ratio; IR, Insulin resistance; LDL, Low-density lipoprotein; LDL-C, Low-density lipoprotein cholesterol; NOS, Newcastle-Ottawa Scale; RR, Risk ratio; TG, Triglyceride. * Corresponding author. E-mail address: Fanzhongjie@pumch.cn (Z. Fan). 1Yuxiong Chen and Zhen’ge Chang contributed equally to this work. https://doi.org/10.1016/j.numecd.2021.11.005 0939-4753/ª 2021 The Italian Diabetes Society, the Italian Society for the Study of Atherosclerosis, the Italian Society of Human Nutrition and the Department of Clinical Medicine and Surgery, Federico II University. Published by Elsevier B.V. All rights reserved.
A systematic review 319 Introduction heartdisease’OR‘coronaryheartdisease’OR‘coronaryartery disease’ OR ‘acute coronary syndrome’ OR ‘myocardial infarction’ OR ‘angina’ OR ‘stroke’ OR ‘cerebrovascular dis- ease’ OR ‘cerebrovascular accident’ OR ‘mortality’ OR ‘death’ AND (3)‘cohort’ OR ‘follow-up’ OR ‘followed up’ OR ‘longi- tudinal’ OR ‘baseline’ in the combination of medical subject headings and text. We first searched PubMed and then tailored the search strategy for each of the other databases. The reference lists of relevant articles were also scanned manually to identify any remaining studies. Cardiovascular disease (CVD) remains one of the leading causes of mortality worldwide [1]. It is well-documented that lowering low-density lipoprotein cholesterol (LDL-C) plays a crucial role in the primary prevention of CVD [2]. However, after the reduction to guideline-recommended levels of LDL-C, a high residual CVD risk still exists due to other lipid components, such as triglyceride (TG) and high-density lipoprotein cholesterol (HDL-C) [3,4]. Several studies have reported that the combination of high TG and low HDL-C level was a predictor of CVD independent of LDL-C level [5e7]. Moreover, combining the two lipid measures into one as the ratio of TG to HDL-C has been proved to be a reliable indicator for insulin resistance (IR) [8,9], which is strongly associated with CVD [10,11]. Compared with the hyperinsulinemic-euglycemic clamp test or the plasma insulin in the homeostasis model assessment of IR, the TG/HDL-C ratio, a parameter calcu- lated from standard lipid profile, is more accessible in real- world clinical practice. The logarithm of TG/HDL-C ratio is also widely used to assess the plasma atherogenicity and is known as the atherogenic index of plasma for a strong correlation with smaller low-density lipoprotein (LDL) particles and increased fractional esterification rate for cholesterol in plasma [12,13]. To date, several cohort studies have explored the as- sociation between the TG/HDL-C ratio at baseline and the incidence of CVD events in the general population [5,14e25]. This study aimed to systematically examine the potential independent association between the TG/HDL-C ratio at baseline and the future risk of CVD events in the general population. We hypothesized that a higher base- line TG/HDL-C ratio would be associated with an increased risk of CVD events. It would be of substantial clinical benefit for early identification and timely intervention of high-risk individuals with elevated TG/HDL-C ratios before developing manifest CVD. Study selection The initial inclusion criteria were: (1) prospective or retrospective cohort studies published as full-length arti- cles; (2) participants from the general population; (3) the TG/HDL-C ratio as exposure of interest measured at base- line; (4) CVD incidence and/or CVD death as outcomes of interest; (5) providing at least age- and sex-adjusted hazard ratio (HR) or risk ratio (RR) with corresponding 95% confidence intervals (CIs). CVD was defined as a composite of coronary heart disease (CHD), stroke and peripheral vascular disease. CHD was defined as myocar- dial infarction, angina pectoris, and other ischemic heart diseases. We excluded: (1) studies that solely enrolled participants with specific diseases (e.g. CHD, chronic kid- ney disease, diabetes, etc) or with high clinical suspected CHD presenting for coronary angiography at baseline, whereas the included studies may have part of partici- pants with such diseases; (2) reported risk estimates by log-transformed TG/HDL-C ratio; (3) only reported risk estimates for all-cause mortality. If several papers reported associations from the same cohort, we only included the study with the longest follow-up period or one with the largest sample size. Two independent reviewers (Ya.Z. and J.F.) initially screened titles and abstracts from all records to identify potentially eligible studies. Full texts were then reviewed to ensure their eligibility for final inclusion. The reviewers compared results and settled discrepancies by discussion and consultation with a third reviewer (Y.C.). Methods We conducted the present meta-analysis following the reporting checklist of the Meta-analysis of Observational StudiesinEpidemiologyStatement[26].Theprotocolforthis systematic review and meta-analysis has been registered at the International Prospective Registerof Systematic Reviews (PROSPERO registration number: CRD42021244583). Data extraction and quality assessment Two investigators (Yong.Z. and Yan.L.) completed the data extraction independently and conflicts were adjudicated by a third investigator (Z.C.). We used a standardized form for data extraction, including the information as follows: article title, first author, year of publication, geographical location, study design, sample sizes, gender distribution, age at baseline, cutoff values of TG/HDL-C ratio compari- son, outcomes and number of events, maximum-adjusted risk estimates (HR or RR) and their corresponding 95% CIs, duration of follow-up, and covariates adjusted in the multivariate analysis. We assessed the study quality using the Newcastle- Ottawa Scale (NOS) of cohort studies according to the se- lection of the study groups, comparability of the groups, and ascertainment of the outcome of interest [27]. This Data sources and searches Weperformedasystematicliteraturesearchofthefollowing electronic bibliographic databases: PubMed, Embase and WebofSciencefromtheirinceptiontoApril11,2021without language restrictions. The termsappliedtoretrieve potential articles for inclusion were: (1)‘triglyceride/high-density li- poprotein cholesterol ratio’ OR ‘triglyceride to high-density lipoprotein cholesterol ratio’ OR ‘TG/HDL-C’ OR ‘TG/HDL cholesterol’ AND (2)‘cardiovascular disease’ OR ‘cardiovas- cular events’ OR ‘cardiovascular outcomes’ OR ‘ischemic
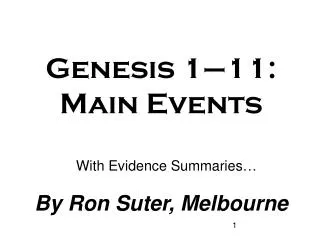
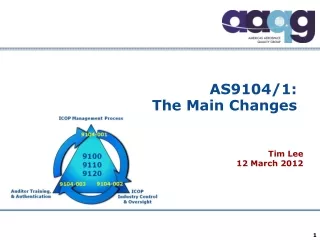
320 Y. Chen et al. Results scale awards a maximum of nine stars to each study. Studies achieving >7 stars were considered high quality. Two independent reviewers (Yi.L. and Z.C.) assessed the quality of the included studies independently. Any disagreement was discussed and resolved by consensus or arbitration by a third reviewer (Y.C.). Literature retrieval Fig. 1 shows the process of the database search. We initially retrieved a total of 565 articles from the system- atic literature searches and 1 from reference lists in the relevant articles. 334 remained after excluding duplicates. By screening the titles and abstracts, 28 studies were considered candidates for inclusion according to the eligibility assessment. Finally, we identified 13 articles included in the meta-analysis after reading full texts [5,14e25]. Data synthesis and analysis The primary outcome was composite CVD events (as defined above). For each outcome, the association be- tween the TG/HDL-C ratio and the risk of CVD was rep- resented by HR. If a study reported several multivariate- adjusted models, the risk estimates from the most adjusted models were applied to minimize the scope for confounding. The reported HRs were classified into two types, categorical TG/HDL-C ratio and continuous TG/ HDL-C ratio. Meta-analysis of categorical risk estimates pooled HRs for the highest TG/HDL-C ratio group versus the reference lowest TG/HDL-C ratio group. For studies with the TG/HDL-C ratio analyzed as a continuous vari- able, we pooled the HRs reported as per unit increase in the TG/HDL-C ratio. A subset of studies also reported risk estimates separately on the secondary CVD outcomes, including CHD events, CHD mortality, myocardial infarc- tion and stroke. We also pooled the risk estimates of the TG/HDL-C ratio (categorical variable) for each CVD sec- ondary outcome. Accounting for significant heterogeneity among the included studies due to geographical locations and characteristics of partici- pants, the study-specific risk estimates were synthe- sized using a prespecified (DerSimonian-Laird method) for more conservative ef- fects [28]. Forest plots were used to illustrate the pooled HRs and 95% CIs. Heterogeneity among the studies was evaluated by Cochran’s Q-statistic test and the extent of inconsistency was assessed by the I2statistic. A p-value < 0.1 or I2>50% suggest the presence of statistically significant heterogeneity [29]. To estimate the potential publication bias, the funnel plot, Begg’s test and Egger’s test were conducted. If statistically significant publica- tion bias was found, the “trim and fill” method was applied to impute the number of potentially missing studies and then the adjusted overall effect size was recomputed [30]. Predefined subgroup analyses were conducted by several study-level characteristics, including sex (all male or mixed population), study location (Europe/America or Asia), adjusting other lipid parameters (yes or no), adjusting dia- betes (yes or no) and categories of the TG/HDL-C ratio (two or more than two). We used meta-regression to test for subgroup differences. The duration of follow-up was treated as a continuous variable in the meta-regression. We also performed sensitivity analyses to test the robustness of our results by sequential omission of individual studies [31]. All the data analyses were carried out using Stata 15.0 (Stata Corporation, College Station, Texas, USA). Statistical signifi- cance was defined as a 2-tailed P-value of 0.05. Study characteristics Table 1 shows the summary characteristics of the 13 included studies in our meta-analysis. A total of 207,515 individuals were identified and analyzed. Of these studies published between 1997 and 2020, 12 studies used a prospective design and 1 used a retrospective design. These studies were conducted in Denmark [5], USA [14,16,18,21,23], Iran [15,20], Argentina [17], Greece [19], Sweden [22] and China [24,25]. The sample size of these studies varied from 796 to 96,542. The mean ages of the included participants varied from 44.7 to 68.8 years old, with the proportion of male participants ranging from 33.8 to 100%. The baseline TG/HDL-C ratio was analyzed as a categorical variable in 9 studies [15,17,18,20e25], as a continuous variable in 3 studies [5,14,19], and as both in 1 study [16]. The number of CVD events of individual studies ranged from 51 to 5422. The mean or median follow-up length varied from 6.4 to 40 years. All studies adjusted for both age and sex, except for 4 studies that only adjusted age because all the participants were male [5,15,18,21] and 1 study without any adjustment since all the participants were male recruited at the age of 50 at baseline [22]. The NOS score of all the studies ranged from 6 to 9, indicating moderate to high study quality (Table 2). different study designs, random-effects model Overall analysis Fig. 2 shows the overall estimates of the random-effects meta-analysis. Comparing the individuals in the highest category with those in the lowest category of the TG/HDL- C ratio at baseline, the pooled HR (95% CI) for CVD was 1.43 (1.26, 1.62), I2Z 72.9, P for heterogeneity <0.001 (Fig. 2a). By continuous TG/HDL-C ratio, the pooled HR (95% CI) for CVD associated with per unit increase in the TG/HDL-C ratio was 1.08 (1.04, 1.12), heterogeneity Z 0.028 (Fig. 2b). The sensitivity analyses by removing one study each time revealed similar results with the original findings (HRs for the TG/HDL-C ratio analyzed as a categorical variable: 1.32e1.49, all P <0.05; HRs for the TG/HDL-C ratio analyzed as a continuous var- iable: 1.06e1.11, all P <0.05) (Fig. 3). Table 2 shows the meta-analysis of the association between the TG/HDL-C ratio (categorical variable) and secondary CVD outcomes. Except for CHD events, a higher TG/HDL-C ratio tends to I2 67.0%, P for Z
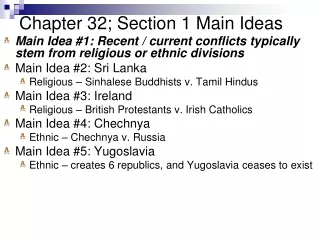
A systematic review 321 Fig. 1 Flowchart of the database search and study identification. significantly increase the risk of secondary CVD outcomes, including CHD death, myocardial infarction and stroke. However, owing to the small number of studies involved in each secondary outcome, the results should be interpreted with caution. More further studies are warranted to elucidate the specific associations. (continuous variable). Interestingly, we found that the risk of CVD was significantly higher in the group without adjustment for other lipid parameters (HR Z 1.72, 95%CI: 1.43e2.08) than in the group with adjustment for other lipid parameters (HR Z 1.21, 95%CI: 1.14e1.29, P for interaction Z 0.008 from meta-regression). This was the only significant heterogeneity we observed among all subgroup analyses in our study. We did not perform sub- group analyses for the TG/HDL-C ratio analyzed as a continuous variable because of the limited number of studies. Subgroup analysis Table 3 presents the subgroup analyses of the primary outcome, showing that the significant relationship be- tween the TG/HDL-C ratio and CVD in the general popu- lation was consistently observed in each predefined subgroup. There were no significant differences in the strength of association according to the sex of population, geographical region, adjustment for diabetes and cate- gories of the TG/HDL-C ratio (all P for interaction >0.05 from meta-regression). Meta-regression showed no significant correlation (P Z 0.820) between the risk of CVD events and the duration of follow-up Publication bias The funnel plot depicting the association between the TG/ HDL-C ratio analyzed as a categorical variable and CVD is shown in Fig. 4. Asymmetric distribution in the funnel plot suggested a high risk of publication bias. Also, Begg’s test (P Z 0.049) and Egger’s test (P Z 0.011) revealed signifi- cant publication bias. The “trim-and-fill” method showed analysis also
322 Table 1 Characteristics of the included studies. Study Country Study design Sample size (% men) Age (years) Cut-off values of TG/ HDL-C ratio Outcome Event number/HR or RR (95% CI) Adjustment for covariates Follow-up (years) Jeppesen (1997) [5] Denmark PC 2910 (100) 63 (range: 53e74) Per unit increase Fatal or non-fatal IHD events Total: 234 1.23 (1.10, 1.37) Age, alcohol consumption, smoking, physical activity, BMI, hypertension, SBP, DBP, NIDDM, social class and TC Age, sex, SBP, anti- hypertensive treatment, diabetes, smoking, and insulin resistance Age, SBP, waist circumference and diabetes 8 Kannel (2008) [14] USA PC 3014 (45) 54 ? 10 Per SD increase CHD events (MI, stable and unstable angina pectoris, or CHD death) CHD events (MI, new-onset angina or CHD death) Incident MI Total: 112 1.26 (1.09, 1.47) 6.4 (mean) Hadaegh (2009) [15] Iran PC 1824 (100) 55 ? 10.6 >6.87 vs. <2.78 Total: 163 1.75 (1.02, 3.00) 6.5 (median) Willey (2011) [16] USA PC 2738 (36.7) 68.8 ? 10.4 >2 vs. ?2/Per unit increase Total: 163 >2 vs. ?2: 1.85 (1.25, 2.74); Per unit increase: 1.06 (1.04, 1.09) Age, sex, race/ethnicity, education, hypertension, diabetes, waist circumference, tobacco use, valvular heart disease, moderate alcohol consumption, cholesterol medication use and physical activity Age, sex, diabetes, TC and number of cigarettes 8.9 (mean) Salazar (2013) [17] Argentina PC 796 (33.8) 51 ? 16 Women: >2.5 vs. ?2.5; Men >3.5 vs. ?3.5 CVD events (angina pectoris, MI, myocardial revascularization and fatal or non- fatal stroke) CVD mortality and CHD mortality Total: 51 1.79 (1.02, 3.21) 8.0 (mean) Vega (2014) [18] USA PC 39,447 (100) 44.7 (range: 20e90) ?3.5 vs. <3.5 Total: 1580 CVD mortality: 1.15 (1.00, 1.33); CHD mortality: 1.30 (1.09, 1.56) Total: 317 1.055 (1.031, 1.078) Age, BMI, SBP, smoking and non-HDL-C 14.7 (mean) Nomikos (2015) [19] Greece PC 2020 (50) 45 ? 14 Per unit increase Fatal or non-fatal CVD events (MI, angina pectoris, other identified forms of ischemia) Age, sex, BMI, physical activity and smoking, MedDietScore, history and management of hypertension, dyslipidemia and diabetes and family history of CVD Age, sex, diabetes, TC and current smoker 8.41 (mean) Gharipour (2016) [20] Iran PC 5431 (48.7) 51.1 ? 11.8 3.68 CVD events (nonfatal and fatal coronary events and stroke, sudden cardiac death, unstable angina) Total: 705 1.29 (1.11, 1.52) 10.9 (median) Y. Chen et al.
A systematic review Farrell (2017) [21] USA PC 40,269 (100) 44.8 ? 9.7 >3.90 vs. <1.51 CHD mortality Total: 556 2.19 (1.69, 2.83) Age, examination year, smoking and family history of heart attack or stroke None 16.6 (mean) Lind Sweden PC 1728 (100) All 50 >1.8 vs. <1.8 CVD events (non- fatal and fatal MI and ischemic stroke) Total: 576 1.46 (1.22, 1.75); MI: 407 1.56 (1.26, 1.92); Ischemic stroke: 258 1.25 (0.94, 1.65) Total: 111 1.51 (0.98, 2.35) 40 (2018) [22] Yang (2019) [23] USA RC 1428 (41.7) 63.6 (range: 56.2 e71.5) Women: ?2.5 vs. <2.5; Men: ?3.5 vs. <3.5 CVD events (MI, angina, CAD, PCI or CABG, stroke, or PVD) Age, sex, race, social- economic status, BMI, smoking, family history of CVD, diabetes, and hypertension Age, sex, smoking, alcohol consumption, education, physical exercise, diabetes, hypertension, TC, LDL-C, heart rate, hs-CRP, BMI, antidiabetic drug therapy, and antihypertensive drug therapy Age, sex, urban or rural residence, northern or southern China, occupational type, education, exercise, smoking, drinking, BMI, hypertension, high LDL-C, diabetes, and antihypertensive medication use 8.1 (median) Chen (2020) [24] China PC 96,542 (79.6) 51.5 ? 12.6 >0.8533 vs. ?0.8533 CVD events (MI and stroke) Total: 5422 1.19 (1.12, 1.26); MI: 1312 1.50 (1.33, 1.70); Stroke: 4228 1.11 (1.03, 1.18) 9.75 (mean) Zhou (2020) [25] China PC 9368 (49.0) 45.8 ? 6.0 >2.10 vs. <1.26 ASCVD events (CHD and ischemic stroke) Total: 624 1.36 (1.10, 1.67); CHD: 177 1.14 (0.78, 1.67); Ischemic stroke: 462 1.47 (1.15, 1.87) 20.3 (median) TG: triglyceride; HDL-C: high-density lipoprotein cholesterol; PC: prospective cohort; RC: retrospective cohort; SD: standard deviation; IHD: ischemic heart disease; CHD: coronary heart disease; MI: myocardial infarction; CVD: cardiovascular diseases; HR: hazard ratio; RR: risk ratio; CI: confidence interval; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting; PVD: peripheral vascular disease; ASCVD: arteriosclerotic cardiovascular disease; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; NIDDM: noninsulin-dependent diabetes mellitus; TC: total cholesterol; LDL-C: low-density lipoprotein cholesterol; hs-CRP: high-sensitivity C-reactive protein. 323
324 Y. Chen et al. that imputing five potential missing studies did not change the significance and direction of association (pooled HR Z 1.26, 95%CI: 1.11e1.44, P <0.001) (Fig. 5). Publication bias for the meta-analysis of the TG/HDL-C ratio analyzed as a continuous variable was difficult to estimate because a limited number of studies was included. Table 2 Meta-analysis of the association between the TG/HDL-C ratio (categorical variable) and secondary CVD outcomes in the general population. Secondary CVD outcomes Studies, n HR (95% CI) Heterogeneity I2, % P CHD events CHD mortality stroke myocardial infarction 2 2 3 3 1.35 (0.89, 2.04) 1.67 (1.00, 2.79) 1.23 (1.03, 1.47) 1.54 (1.39, 1.70) 0.203 0.001 0.074 0.598 38.2% 90.6% 61.6% 0.0% Discussion In this systematic review and meta-analysis of cohort studies, compared with the participants with the bottom category of the TG/HDL-C ratio, those with the top cate- gory were independently associated with an increased risk TG: triglyceride; HDL-C: high-density lipoprotein cholesterol; CVD: cardiovascular diseases; HR: hazard ratio; CI: confidence interval; CHD: coronary heart disease. Fig. 2 analyzed as a categorical variable. b. Meta-analysis with the TG/HDL-C ratio analyzed as a continuous variable. HR, hazard ratio; CI, confidence interval. Forest plots for the meta-analysis of the association between the TG/HDL-C ratio and CVD events. a. Meta-analysis with the TG/HDL-C ratio
A systematic review 325 Fig. 3 the TG/HDL-C ratio analyzed as a categorical variable (HR ranges: 1.32e1.49). b. Sensitivity analysis with the TG/HDL-C ratio analyzed as a continuous variable (HR ranges: 1.06e1.11). HR, hazard ratio; CI, confidence interval. Sensitivity analyses for the meta-analysis of the TG/HDL-C ratio and CVD events (given name study is omitted). a. Sensitivity analysis with of CVD in the general population. After adjusting for publication bias using the “trim and fill” method, the pooled effect remained positive and significant. A meta- analysis with the TG/HDL-C ratio analyzed as a contin- uous variable also confirmed the robustness of findings. Sensitivity analyses were performed to highlight the sta- bility of the findings, which were not driven by an indi- vidual study. Although the included studies varied in terms of population gender, geographical region, length of follow-up, adjustment for diabetes, adjustment for other lipid parameters and categories of the TG/HDL-C ratio, none of these study-level characteristics significantly affected the significance or direction of effects for the as- sociation between the TG/HDL-C ratio with CVD events. All these findings suggested that a higher TG/HDL-C ratio at baseline may be an independent predictor of an increased risk of CVD in the general population. Thus, healthcare workers should pay more attention to the TG/
326 Y. Chen et al. Table 3 Subgroup analyses of the TG/HDL-C ratio (categorical variable) with CVD events in the general population. Subgroups Studies, n HR (95% CI) Heterogeneity P for interaction I2, % P Sex men men and women Geographic location Europe/America Asia Adjusted for other lipid parameters Yes No Adjusted for diabetes Yes No Categories of the TG/HDL-C ratio two three or more 4 6 1.55 (1.16, 2.09) 1.32 (1.18, 1.49) 0.000 0.105 84.8% 45.0% 0.558 6 4 1.58 (1.26, 1.99) 1.25 (1.14, 1.35) 0.001 0.271 77.1% 23.4% 0.249 5 5 1.21 (1.14, 1.29) 1.72 (1.43, 2.08) 0.352 0.143 9.6% 41.8% 0.008 7 3 1.35 (1.19, 1.51) 1.52 (1.09, 2.13) 0.097 0.000 44.1% 89.5% 0.132 7 3 1.30 (1.18, 1.44) 1.72 (1.21, 2.44) 0.051 0.019 52.1% 74.9% 0.734 TG: triglyceride; HDL-C: high-density lipoprotein cholesterol; CVD: cardiovascular diseases; HR: hazard ratio; CI: confidence interval; CHD: coronary heart disease. Fig. 4 Funnel plots for the meta-analysis of the TG/HDL-C ratio (categorical variable) and CVD events. HR, hazard ratio; SE, standard error. HDL-C ratio, especially among people at high risk of CVD. Because TG and HDL-C are routinely examined in clinical practice, the measurement of the TG/HDL-C ratio would not increase the financial burden on patients. As a simple and inexpensive indicator of IR, the TG/HDL-C ratio is also associated with several including diabetes [32], hypertension [33], obesity [34] and hyperuricemia [35]. The usefulness of the TG/HDL-C ratio in predicting the risk of CVD and helping clinical decisions will require formal evaluation by calculation of risk prediction metrics, such as risk discrimination and risk reclassification in further large-scale prospective cohort studies with long follow-up period. Although the benefits from lowering the TG/HDL-C elevated TG level and low HDL-C level are regarded as markers of residual cardiovascular risk beyond LDL-C [36]. Icosapent ethyl, a highly purified eicosapentaenoic acid ethyl ester has been shown to lower TG levels and play a role in reducing CVD risk among patients with elevated TG levels despite statin therapy [37]. Interestingly, we found that adjusting for other lipid parameters (total cholesterol or LDL-C or non-HDL-C) significantly reduced the strength of the relationship be- tween CVD and the TG/HDL-C ratio, suggesting that ratio remain unclear, cardiometabolic diseases,
A systematic review 327 Fig. 5 Filled funnel plots for the meta-analysis of the TG/HDL-C ratio (categorical variable) and CVD events. SE, standard error. adjustment for other lipid parameters may be one of the sources of heterogeneity. It is consistent with a previous study that found further adjustment for TC or LDL-C weakened the effect of one unit increase in the TG/HDL- C ratio on the risk of ischemic heart disease, indicating that part of the association may be mediated through other lipid levels [5]. Future studies are needed to explore whether other lipid parameters could function as an effect modifier in the relationship between the TG/HDL-C ratio and CVD events and the pathogenic mechanism behind such inference. Another individual participant data meta-analysis of 32 cohortstudiesofgeneralpopulationsperformedintheAsia- PacificregionreportedthattheHR(95%CI)ofCVDmortality for one standard deviation higher level of log (TG/HDL-C) was1.21(1.09,1.34)[38].ThemechanismunderlyingtheTG/ HDL-CratiowithCVDeventsremainsunclear.Onepotential explanation is that the TG/HDL-C ratio is highly associated with IR [39], which is the central feature of metabolic syn- drome with several manifestations, including elevated TG and decreased HDL-C [40]. IR has been identified as a well- known risk factor of CVD, playing a role in both athero- genesis and advanced plaque progression [41]. Another explanation is that the TG/HDL-C ratio has a strong corre- lationwithsmalldenseLDLasanatherogenicindexbecause of its susceptibility to oxidative modification [42]. The TG/ HDL-C ratio is negatively associated with the number of larger, more buoyant, less atherogenic LDL particles, whereas positively associated with the amount of small, dense pro-atherogenic LDL particles [43]. To the best of our knowledge, this study is the first literature-based meta-analysis to explore the association between the TG/HDL-C ratio and CVD events in the general population. We only included cohort studies with fully- adjusted risk estimates from general populations; there- fore, the potential recall or selection bias that existed in cross-sectional or case-control studies was avoided. Most of the included studies (10/13) were of high quality ac- cording to the NOS score. All the included studies indi- cated that the TG and HDL-C measurements were determined in fasting status. Although it has been rec- ommended that fasting is not routinely required for the determination of a lipid profile, fasting may be important in patients with very high TG levels, strengthening the accuracy of measurements of the TG/HDL-C ratio [44,45]. Nevertheless, we acknowledged that our study had several limitations that should be considered when inter- preting the results. First, this is a literature-based but not individual participants’ meta-analysis based on a limited number of studies with significant heterogeneity among them. Second, although we used the maximum-adjusted risk estimates from each study to calculate the pooled result, there are still many residual confounding factors that may affect the pooling results, such as the dietary and nutritional factors. Third, a single estimation of the TG/ HDL-C ratio at baseline may have resulted in the misclas- sification of participants in each category of the TG/HDL-C ratio. Fourth, various cut-off values of the TG/HDL-C ratio level were applied in the included studies and we failed to determine the optimal cut-off value in clinical settings for the prediction of future CVD events. Last, the results of subgroup analyses may be unreliable due to the small number of eligible studies. Conclusions The current meta-analysis indicates that a higher TG/HDL- C ratio is independently associated with CVD risk in the
328 Y. Chen et al. general population. As a reliable and convenient marker of IR in clinical settings, the TG/HDL-C ratio is of great po- tential use in the prediction and prevention of CVD. Further well-designed cohort studies or interventional studies are warranted to support these findings, to explore the optimal cut-off values and the shape of a dose- response relationship, and to assess whether lowering TG/HDL-C ratio can bring cardiovascular benefits to the general population. ischemic heart disease - an 8-year follow-up in the Copenhagen Male Study. Arterioscler Thromb Vasc Biol 1997;17:1114e20. [6] Lee JS, Chang PY, Zhang Y, Kizer JR, Best LG, Howard BV. Triglyceride and HDL-C dyslipidemia and risks of coronary heart disease and ischemic stroke by glycemic dysregulation status: the Strong Heart Study. Diabetes Care 2017;40:529e37. [7] Andersson C, Lyass A, Vasan RS, Massaro JM, D’Agostino Sr RB, Robins SJ. Long-term risk of cardiovascular events across a spec- trum of adverse major plasma lipid combinations in the Framing- ham Heart Study. Am Heart J 2014;168:878e883.e1. [8] Young KA, Maturu A, Lorenzo C, Langefeld CD, Wagenknecht LE, Chen YI, et al. The triglyceride to high-density lipoprotein choles- terol (TG/HDL-C) ratio as a predictor of insulin resistance, b-cell function, and diabetes in Hispanics and African Americans. J Diabet Complicat 2019;33:118e22. [9] Tjokroprawiro A, Dwi Suryantoro S, Murtiwi S, Sutjahjo A, Wibisono S, Pranoto A, et al. Triglycerides/HDL-cholesterol ratio is correlated with insulin resistance in patients with type 2 diabetes mellitus. Diabetes Res Clin Pract 2014;106:S91e2. [10] Bonora E, Kiechl S, Willeit J, Oberhollenzer F, Egger G, Meigs JB, et al. Insulin resistance as estimated by homeostasis model assessment predicts incident symptomatic cardiovascular disease in caucasian subjects from the general population: the Bruneck study. Diabetes Care 2007;30:318e24. [11] Hanley AJ, Williams K, Stern MP, Haffner SM. Homeostasis model assessment of insulin resistance in relation to the incidence of cardiovascular disease: the San Antonio Heart Study. Diabetes Care 2002;25:1177e84. [12] Dobiásová M, Frohlich J. The plasma parameter log (TG/HDL-C) as an atherogenic index: correlation with lipoprotein particle size and esterification rate in apoB-lipoprotein-depleted plasma (FER(HDL)). Clin Biochem 2001;34:583e8. [13] Frohlich J, Dobiásová M. Fractional esterification rate of cholesterol and ratio of triglycerides to HDL-cholesterol are powerful pre- dictors of positive findings on coronary angiography. Clin Chem 2003;49:1873e80. [14] Kannel WB, Vasan RS, Keyes MJ, Sullivan LM, Robins SJ. Usefulness of the triglyceride-high-density lipoprotein versus the cholesterol- high-density lipoprotein ratio for predicting insulin resistance and cardiometabolic risk (from the Framingham Offspring Cohort). Am J Cardiol 2008;101:497e501. [15] Hadaegh F, Khalili D, Ghasemi A, Tohidi M, Sheikholeslami F, Azizi F. Triglyceride/HDL-cholesterol ratio is an independent pre- dictor for coronary heart disease in a population of Iranian men. Nutr Metabol Cardiovasc Dis 2009;19:401e8. [16] Willey JZ, Rodriguez CJ, Carlino RF, Moon YP, Paik MC, Boden- Albala B, et al. Race-ethnic differences in the association between lipid profile components and risk of myocardial infarction: the Northern Manhattan Study. Am Heart J 2011;161:886e92. [17] Salazar MR, Carbajal HA, Espeche WG, Aizpurúa M, Leiva Sisnieguez CE, March CE, et al. Identifying cardiovascular disease risk and outcome: use of the plasma triglyceride/high-density li- poprotein cholesterol concentration ratio versus metabolic syn- drome criteria. J Intern Med 2013;273:595e601. [18] Vega GL, Barlow CE, Grundy SM, Leonard D, DeFina LF. Triglycer- ide-to-high-density-lipoprotein-cholesterol ratio is an index of heart disease mortality and of incidence of type 2 diabetes mel- litus in men. J Invest Med 2014;62:345e9. [19] Nomikos T, Panagiotakos D, Georgousopoulou E, Metaxa V, Chrysohoou C, Skoumas I, et al. Hierarchical modelling of blood lipids’ profile and 10-year (2002-2012) all cause mortality and incidence of cardiovascular disease: the ATTICA study. Lipids Health Dis 2015;14:108. [20] Gharipour M, Sadeghi M, Dianatkhah M, Nezafati P, Talaie M, Oveisgharan S, et al. Comparison between European and Iranian cutoff points of triglyceride/high-density lipoprotein cholesterol concentrations in predicting cardiovascular disease outcomes. J Clin Lipidol 2016;10:143e9. [21] Farrell SW, Finley CE, Barlow CE, Willis BL, DeFina LF, Haskell WL, et al. Moderate to high levels of cardiorespiratory fitness attenuate the effects of triglyceride to high-density lipoprotein cholesterol ratio on coronary heart disease mortality in men. Mayo Clin Proc 2017;92:1763e71. [22] Lind L, Ingelsson E, Ärnlöv J, Sundström J, Zethelius B, Reaven GM. Can the plasma concentration ratio of triglyceride/high-density Funding This work was supported by Chinese Academy of Medical Sciences (CAMS) Initiative for Innovative Medicine [grant number 2017-I2M-2-001]; Foundation [grant number 91643208]; and National Key Research and Development Plan [grant number 2017YF C0211703]. National Natural Science Authors’ contributions Y.C., Z.C. and Z.F. conceived and designed research; Yi.L., Ya.Z., J.F., Yong. Z. and Yan.L. collected the data. Y.C., Z.C. and Yi.L. analyzed and interpreted data; Y.C. and Z.C. drafted the initial manuscript; Z.F. reviewed and revised the paper. All authors have read and approved the final manuscript. Declaration of competing interest The authors declared they do not have anything to disclose regarding conflict of interest for the manuscript. Acknowledgments Not applicable. Appendix A. Supplementary data Supplementary data to this article can be found online at https://doi.org/10.1016/j.numecd.2021.11.005. References [1] Collaborators GDaI. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England) 2020;396:1204e22. [2] Tokgozoglu L, Kocyigit D. Should we target global risk or risk fac- tors? Curr Atherosclerosis Rep 2021;23:2. [3] Sampson UK, Fazio S, Linton MF. Residual cardiovascular risk despite optimal LDL cholesterol reduction with statins: the evi- dence, etiology, and therapeutic challenges. Curr Atherosclerosis Rep 2012;14:1e10. [4] Carey VJ, Bishop L, Laranjo N, Harshfield BJ, Kwiat C, Sacks FM. Contribution of high plasma triglycerides and low high-density li- poprotein cholesterol to residual risk of coronary heart disease after establishment of low-density lipoprotein cholesterol control. Am J Cardiol 2010;106:757e63. [5] Jeppesen J, Hein HO, Suadicani P, Gyntelberg F. Relation of high TG low HDL cholesterol and LDL cholesterol to the incidence of
A systematic review 329 lipoprotein cholesterol identify individuals at high risk of cardio- vascular disease during 40-year follow-up? Metab Syndr Relat Disord 2018;16:433e9. [23] Yang M, Rigdon J, Tsai SA. Association of triglyceride to HDL cholesterol ratio with cardiometabolic outcomes. J Invest Med 2019;67:663e8. [24] Chen Z, Chen G, Qin H, Cai Z, Huang J, Chen H, et al. Higher tri- glyceride to high-density lipoprotein cholesterol ratio increases cardiovascular risk: 10-year prospective study in a cohort of Chi- nese adults. J Diabetes Investig 2020;11:475e81. [25] Zhou L, Mai J, Li Y, Guo M, Wu Y, Gao X, et al. Triglyceride to high- density lipoprotein cholesterol ratio and risk of atherosclerotic cardiovascular disease in a Chinese population. Nutr Metabol Cardiovasc Dis 2020;30:1706e13. [26] Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000;283:2008e12. [27] Wells G, Shea B, O’Connell D, Peterson j, Welch V, Losos M, et al. The NewcastleeOttawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. 2000. http://www. ohri.ca/programs/clinical_epidemiology/oxford.asp. [28] DerSimonian R, Laird N. Meta-analysis in clinical trials. Contr Clin Trials 1986;7:177e88. [29] Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ (Clin Res Ed) 2003;327: 557e60. [30] Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta- analysis. Biometrics 2000;56:455e63. [31] Patsopoulos NA, Evangelou E, Ioannidis JP. Sensitivity of between- study heterogeneity in meta-analysis: proposed metrics and empirical evaluation. Int J Epidemiol 2008;37:1148e57. [32] Kim J, Shin SJ, Kim YS, Kang HT. Positive association between the ratio of triglycerides to high-density lipoprotein cholesterol and diabetes incidence in Korean adults. Cardiovasc Diabetol 2021;20: 183. [33] Liu D, Guan L, Zhao Y, Liu Y, Sun X, Li H, et al. Association of tri- glycerides to high-density lipoprotein-cholesterol ratio with risk of incident hypertension. Hypertens Res 2020;43:948e55. [34] Zhu X, Yu L, Zhou H, Ma Q, Zhou X, Lei T, et al. Atherogenic index of plasma is a novel and better biomarker associated with obesity: a population-based cross-sectional study in China. Lipids Health Dis 2018;17:37. [35] Yu Y, Lan T, Wang D, Fang W, Tao Y, Li M, et al. The association of lipid ratios with hyperuricemia in a rural Chinese hypertensive population. Lipids Health Dis 2021;20:121. [36] Libby P. Triglycerides on the rise: should we swap seats on the seesaw? Eur Heart J 2015;36:774e6. [37] Bhatt DL, Steg PG, Miller M, Brinton EA, Jacobson TA, Ketchum SB, et al. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med 2019;380:11e22. [38] Barzi F, Patel A, Woodward M, Lawes CM, Ohkubo T, Gu D, et al. A comparison of lipid variables as predictors of cardiovascular dis- ease in the Asia Pacific region. Ann Epidemiol 2005;15:405e13. [39] Giannini C, Santoro N, Caprio S, Kim G, Lartaud D, Shaw M, et al. The triglyceride-to-HDL cholesterol ratio: association with insulin resistance in obese youths of different ethnic backgrounds. Dia- betes Care 2011;34:1869e74. [40] Grundy SM. Hypertriglyceridemia, insulin resistance, and the metabolic syndrome. Am J Cardiol 1999;83. 25f-9f. [41] Bornfeldt KE, Tabas I. Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metabol 2011;14:575e85. [42] Maruyama C, Imamura K, Teramoto T. Assessment of LDL particle size by triglyceride/HDL-cholesterol ratio in non-diabetic, healthy subjects without prominent hyperlipidemia. J Atherosclerosis Thromb 2003;10:186e91. [43] Hanak V, Munoz J, Teague J, Stanley Jr A, Bittner V. Accuracy of the triglyceride to high-density lipoprotein cholesterol ratio for pre- diction of the low-density lipoprotein phenotype B. Am J Cardiol 2004;94:219e22. [44] Nordestgaard BG, Langsted A, Mora S, Kolovou G, Baum H, Bruckert E, et al. Fasting is not routinely required for determina- tion of a lipid profile: clinical and laboratory implications including flagging at desirable concentration cut-points-a joint consensus statement from the European Atherosclerosis Society and European Federation of Clinical Chemistry and Laboratory Medicine. Eur Heart J 2016;37:1944e58. [45] Naugler C, Sidhu D. Break the fast? Update on patient preparation for cholesterol testing. Can Fam Physician 2014;60(895e7):e471e4.