Download
1 / 44
670 likes | 1.77k Views
Using the Patient Health Questionnaire (PHQ-9): The Hgb A-1-C for Depression. Neil Korsen, MD, MS Medical Director, MaineHealth Caring for ME/ Depression in Primary Care Program. Key Points. Depression is a common problem that causes much morbidity and mortality

E N D
Using the Patient Health Questionnaire (PHQ-9): The Hgb A-1-C for Depression Neil Korsen, MD, MS Medical Director, MaineHealth Caring for ME/ Depression in Primary Care Program
Key Points • Depression is a common problem that causes much morbidity and mortality • Most patients treated for depression receive all their treatment in the primary care setting • There is solid evidence that a model of depression care consistent with the Planned Care Model leads to better outcomes for people with depression.
The PHQ-9 • Is a validated tool to screen for and diagnose depression. • Has also been validated as a tool for measuring response to treatment. • Is easy to use and has been found to be helpful by Maine primary care clinicians who have been using it for several years.
What is Watchful Waiting? • It is estimated that a third of people with mild symptoms will recover without treatment. • Watchful waiting means you are seeing the patient about once a month and monitoring their PHQ-9 score, but not starting active treatment. • Self-care activities such as exercise or relaxation are usually a component of watchful waiting. • If the patient’s symptoms have not resolved after 2-3 months, active treatment ought to be considered.
Screening – Who and How US Preventive Services Task Force, 2003 statement supporting screening for depression: (We) recommend screening adults for depression in clinical practices that have systems in place to assure accurate diagnosis, effective treatment, and follow-up. www.ahrq.gov
Screening for Depression: Who do you screen? • All adults at least every 5 years (as part of a health maintenance visit?) • High risk groups every year • History of depression • Family history of depression or bipolar • Chronic illnesses such as diabetes, heart disease, pain problems • High utilization of services • People with complaints that suggest depression such as insomnia or fatigue
Screening for Depression: The first two questions of the PHQ-9 have been validated as a sensitive way to screen for depression • 96% of people with depression will say yes to one of those two questions • Answer of ‘2’ or ‘3’ on either of those questions is a positive screen • Administer the full PHQ-9 to those who screen positive
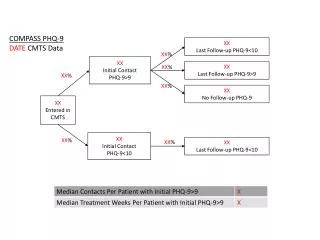
PHQ-9 Depression Assessment Tool The PHQ-9-9 is used in two different ways. Initially to assess patients for depression and subsequently to monitor treatment progress should a formal DX of depression be made. When assessing patients the score of the first two questions will determine whether or not you would need to go forward with the remaining questions. For example if the first two questions score as two or less you will be notified that the patient has screened negative for depression. For patient with a diagnosis of depression all other questions should be answered regardless of score in the first two question.
Things to Consider in Initiating Use of the PHQ-9 in your daily work • How will you identify those patients who should fill out a PHQ? • Who will give the patient the PHQ? • Who will score the PHQ? • Who will enter the results into the registry? When will that be done? • How often should the PHQ be done?
How often should the PHQ be done? • Once a month until the patient reaches remission (score 0-4) or for the first 6 months of treatment • Every 3 months after that while the patient is on active treatment • Once a year for people with a history of depression who are no longer on active treatment
Practice Case #1: Initial Visit • 45 year-old businessman • Feeling tired, not sleeping well lately • A good friend was killed in a car crash a few months ago • Work has been more stressful for the past year • You recognize that his symptoms suggest depression and you ask him to fill out a PHQ-9
Case #1: Questions • What is his PHQ-9 score? • What is his severity level? • Based on his severity level, what would you recommend?
Case #1: 4-week follow-up visit • He returns after 4 weeks • Has been taking medication you prescribed • Had some nausea initially, but that has improved when he started taking the medication with food. • Says he is feeling better • His PHQ-9 today:
Case #1: 4-week follow-up visit • What is his PHQ-9 score today? • How would you describe his response to treatment (good, fair, poor)? • What might you do next?
Case #1: 8-week follow-up visit • He returns in another month • Reports he is feeling much better, almost like his old self • Continues to take the medicine and has not been bothered by side effects • His PHQ-9 score today is:
Case #1: 8-week follow-up visit • What is his score today? • Has he reached remission? • What is your advice about continuing on treatment?
Case #2 • 32 year-old woman • 6 weeks of depressed mood, poor sleep and appetite • Had an episode of depression about 5 years ago, which was successfully treated with Zoloft • Her PHQ-9:
Case #2: Questions • What is her PHQ-9 score? • What is her severity level? • Based on her severity level, what would you recommend?
Case #3 • 28 year-old man • Several weeks of feeling down, trouble concentrating, and frequent awakening at night • You recognize that this might be depression and administer a PHQ-9:
Case #3: Questions • What is his PHQ-9 score? • What is his severity level? • Based on his severity level, what would you recommend?
Case #4 • 74 year-old man • Complaints of fatigue and trouble with his memory • History of hypertension, but is otherwise fairly healthy. • His PHQ score:
Case #4: Questions • What is his PHQ-9 score? • What is his severity level? • Based on his severity level, what would you recommend?
Accessing our e-learn modules • elearn.mmc.org/depression • Sign in either using your MMC login name as your user name and password, or by using welcome as your user name and password.
Depression Collaborative Participants • Portland area: • Bowdoin Medical Group – S. Portland • Andrew Candelore, DO • Joseph DeKay, DO • Maine Med Family Practice Centers • Maine Med Medical Clinic • Maine Med Ob-Gyn Clinic • Sacopee Valley Health Center • Scarborough Family Physicians
Depression Collaborative Participants • Damariscotta area: • Miles Family Medicine/ Damariscotta • Miles Internal Medicine • Augusta area: • Augusta Family Physicians • Capital Family Practice • Gardiner Family Practice • Sheepscot Valley Health Center • Winthrop Health Center
Institute of Medicine “Quality Chasm” Report for Mental Health • Clinicians should: Increase their use of valid and reliable patient questionnaires … that are feasible for routine use to assess the progress and outcomes of treatment systematically and reliably.
Paying for the PHQ-9 • The National Business Group on Health (a group of more than 200 large employers): • “Monitor patient progress with standardized, evidence-based instruments. Reimburse patient monitoring as a lab test.” • Aetna is piloting paying for the PHQ-9. • We are negotiating to be included in that pilot.
References • ‘Improving the Quality of Health Care for Mental and Substance-Use Conditions’, Institute of Medicine, 2006. Accessed at http://fermat.nap.edu/catalog/11470.html, 6/2/06 • ‘An Employer’s Guide to Behavioral Health Services’, National Business Group on Health, 2005. Accessed at http://64.78.6.200/prevention/et_behavioralhealthreport.cfm?%20Health%20Services:%20Tools%20and%20Solutions%20-%20&, 6/2/06 • Spitzer, Kroenke et al, JAMA, 1999, V.282, pp.1737-44. • Lowe, Unutzer et al, Medical Care, 2004, V.42, pp. 1194-1201.