Download
1 / 5
50 likes | 69 Views
Infant Dyschezia NHS is an umbrella term that encompasses a group of disorders associated with persistent difficulty , infrequent or seemingly incomplete defecation without evidence of a structural or biochemical explanation<br>

E N D
Infant Dyschezia NHS a4medicine.co.uk
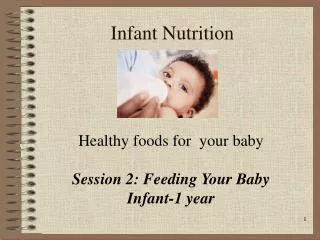
What is constipation – currently the most widely accepted definitions for childhood functional constipation are the Rome III definitions. These are different based on age groups Functional constipation is an umbrella term that encompasses a group of disorders associated with persistent difficulty , infrequent or seemingly incomplete defecation without evidence of a structural or biochemical explanation (Manu R Sood , FRCPCH. MD ref 5 )Age < 4 yrs No organic pathology & 2 or more of the following for atleast 1 month-Two or < 2 defecations / week At least 1 episode of incontinence / week after the acquisition of toileting skills H/O excessive stool retention H/O painful or hard bowel movements Presence of a large faecal mass in the rectum H/O large-diameter stools that may obstruct the toiletAge > 4 yrs Insufficient criteria for irritable bowel syndrome Criteria fulfilled atleast once/ week for atleast 2 months before diagnosis Two or < 2 defaecations / week At least episode of fecal incontinence / week H/O retentive posturing or excessive volitional stool retention H/O painful or hard bowel movements Presence of large fecal mass in the rectum H/O large diameter stools that may obstruct the toiltAbdominal pain is a frequent associated symptom but its presence is not considered a criterion for functional constipation Infant dyschezia NHS – a sub group of children has defecation-related difficulties and has been sub-categorized according to the Rome III has having ” infant dyschezia “. This is described as ○ occurring in infants > 6 months○ atleast 10 minutes of straining and crying before successful passage of soft stools ○ no other health problemsChildhood constipation is very common Nearly all childhood constipation is functional but 5-10 % are due to an organic cause Accounts for up to 25 % of referrals to tertiary pediatric OP clinics Responsible for 3-5 % of paediatric primary care visits Peak incidence is at the time of toilet training Peak incidence between ages 2-4 yrs Gender differences not clear although some papers mention it to be ↑↑ in girls Prevalence varies widely○ In the UK 10-20 % ( Auth et al, 2002 )○ Worldwide 0.8 % to 28 %○ Lowest in Finland highest in USA a4medicine.co.uk
Cause unclear – possibly multifactorial Withholding behaviour – often starts with a painful frightening bowel movement -> stool remains in rectum –> rectal mucosa rebsorbs water from retained stool –> becomes more difficult to evacuate –> vicious cycle –> faecal impaction , loss of rectal sensationand ultimately loss of normal urge to defaecate Diet Slow transit Family history ie genetic factors may play a role Toilet training Some behaviour conditions as autism and ADHD Children with underlying bladder dysfunction Parental-child rearing attitudes Stress ( e.g child abuse )Organic causes of constipation in children include metabolic , endocrine disorders , anorectal anomalies , neuromuscular disroders or Hirschsprung’s diseaseHistory-What do parents mean by constipation Delay in passage of meconium Toilet history -Frequency , consistency , soiling , blood , pain Age at onset Abdominal pain -between 10-70 % of children with constipation c/o non-specific abdominal pain Faecal incontinence ( impaction , overflow ) Diet and fluid intake ( e.g with cow’s milk ) Withholding behavior ( e.g retentive posturing ) Urinary symptoms UTIs and enuresis are reported in 30 % of constipated children Social history Any treatment tried and response Any medication use e.g antacids , opiatesExamination –Physical growth ( eg cystic fibrosis , hypothyroidism→ stunted growth failure to thrive )Height / weight – Plot on chart General examination Abdominal examination ? evidence faecal loading Perineal inspection- ○ particularly infants to r/o anorectal abnormality○ position of anus ( any anotomical anomalies )○ fissures○ tags ( clue to anal fissures )○ inflammation Neurological examination -inspection of spine to exclude spina bifida or cerebral palsy Rectal examination is usually not carried out in primary care and would be done by specialists if they feel it can provide additional information ( for e.g alarm signs present , intractable constipation )Complications –Anal fissure Haemorrhoids Rectal prolapse Megarectum Faecal impaction and soiling Volvulus Distress ,missed school , poor school performance , social isolation a4medicine.co.uk
Red flags-Symptoms appear from birth or during the 1st few weeks of life ( may indicate Hirschsprung’s disease- congenital aganglionic megacolon )Delayed meconium > 48 hrs after birth in a full term baby ( may indicate Hirschsprung’s disease or cystic fibrosis )Abdominal distension with vomiting- may indicate Hirschsprung’s disease or intestinal obstruction ) Family h/o Hirschsprung’s disease Ribbon stool pattern -may indicate anal stenosis likely if child < 1 yr ) Leg weakness or motor delay ( neurological or spinal cord abnormality )Abnormal appearance of anus -○ fistulae ○ bruising ○ fissure ○ tight or patalous-widely patent ○ anteriorly placed anus○ absent anal wink→reflex contraction of the external anal sphincter when the skin around anus is stroked Abnormalities in lumbosacral and gluteal regions○ asymmetry of gluteal muscles○ evidence of sacral agenesis ○ scoliosis○ discolored skin○ naevi○ hairy patch○ sinus or central pitAmber flags- Evidence of faltering growth , developmental delay or indications of a systemic illness ( liaise with specialist to arrange testing for possible Coeliac disease , hypothyroidism ,cystic fibrosis and electrolyte disturbance ) Constipation triggered by the introduction of cow’s milk Child maltreatment concernFaecal impaction –Faecal impaction is defined as a hard mass in the lower abdomen identified on physical examination or a dilated rectum filled with a large amount of stool on rectal examination or excessive stool in the distal colon on abdominal radiography An impaction is present in 30 to 75 % of constipated children and more than 90 % of children with faecal incontinence Majority of constipated children have palpable abdominal masses and/ or fecal impaction of the rectal on physical examination a4medicine.co.uk
Management of Childhood Functional Constipation Lisa Philchi , MN, CPNP The Journal of Pediatric Health Care Jan-Feb 2018 , Volume 32, Issue 1, Pages 103-111 • Levy EI, Lemmens R, Vandenplas Y, Devreker T. Functional constipation in children: challenges and solutions. Pediatric Health Med Ther. 2017;8:19–27. Published 2017 Mar 9. doi:10.2147/PHMT.S110940 • Management of Functional Constipation in Children : Therapy in Practice Koppen, I.J.N., Lammers, L.A., Benninga, M.A. et al. Pediatr Drugs (2015) 17: 349. https://doi.org/10.1007/s40272-015-0142-4 • Childhood Constipation : is There Light in the Tunnel Benninga, M A et al Journal of PediatricGatroenterology and Nutrition Issue : Volume 39 (5), November 2004 , pp 448-464 • Chronic functional constipation and fecalinconctinence in infants and children : Treatment Manu R sood, FRCPCH via Uptodate.com • CKS NHS Constipation in children revised June 2019 • Mistakes in paediatric functional constipation diagnosis and treatment and how to avoid them Marc A Benninga and Daniel R Hoekman UEG education Oct 2016 • Evaluation and Treatment of Functional Constipation in Infants and Children : Evidence – Based Recommendations From ESPGHAN and NASPGHAN JPGN Volume 58, Number 2 , February 2014 References