Download

1 / 24
240 likes | 563 Views
Flexor Tendons - Zones. Extensor Tendons Zones. Diagnosis of Flexor Injury. Normal cascade Independent testing of FDS & FDP Passive tenodesis test Forearm compression test. Flexor Tendon Testing. Normal Flexion Cascade. Tenosynovitis Anatomy. Flexor sheaths are closed spaces

E N D
Diagnosis of Flexor Injury • Normal cascade • Independent testing of FDS & FDP • Passive tenodesis test • Forearm compression test
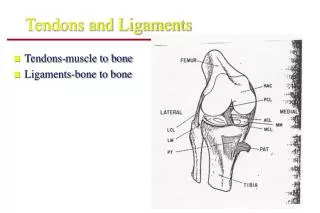
TenosynovitisAnatomy • Flexor sheaths are closed spaces • Extend from the mid-palmar crease to the DIPJ (Prox edge of A1 pulley to distal edge of A5 pulley) • Flexor sheath of small finger is continuous proximally with the Ulnar Bursa, while the sheath of the thumb is continuous with the Radial Bursa • Radial & Ulnar bursae extend proximal to the TCL and connect with the Parona space(Potential space between FDP & PQ muscle)
TenosynovitisGeneral • Flexor sheath infections most often as a result of penetrating trauma • More likely at joint flexion creases • Sheaths are separated from skin by only a small amount of subcutaneous tissue here • Also, Felons can rupture into the distal flexor sheath • Usual causative agent: S. Aureus • most commonly affected digits: • Ring, long & index fingers
TenosynovitisGeneral • Purulence within the sheath destroys the gliding mechanism, rapidly creating adhesions that lead to loss of function • destroys the blood supply producing tendon necrosis
TenosynovitisClinical • Kanavel’s 4 cardinal signs: • Tenderness over & limited to the flexor sheath • Symmetrical enlargement of the digit (“fusiform”) • Severe pain on passive extension of the finger (> proximally) • Flexed posture of the involved digit • Not all four signs may be present early on • Most reliable sign: pain w. passive extension • Cellulitis of the hand may appear similar, but swelling & tenderness is not usually isolated to a single digit
TenosynovitisTreatment • Early infection < 48 hrs (& usually lacking all 4 signs) may initially be treated with IV Abx, splinting & elevation • Failure to respond within 24 hrs. should necessitate drainage • Established pyogenic tenosynovitis is a surgical emergency • Requires prompt surgical drainage • Delays may result in tendon &/or skin necrosis