Download
1 / 1

E N D
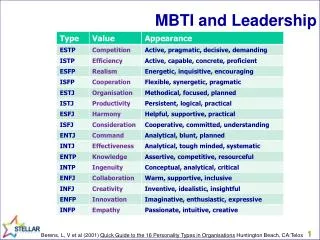
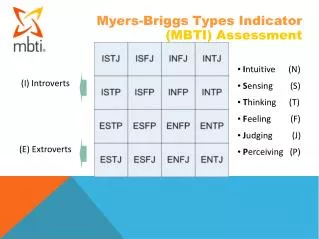
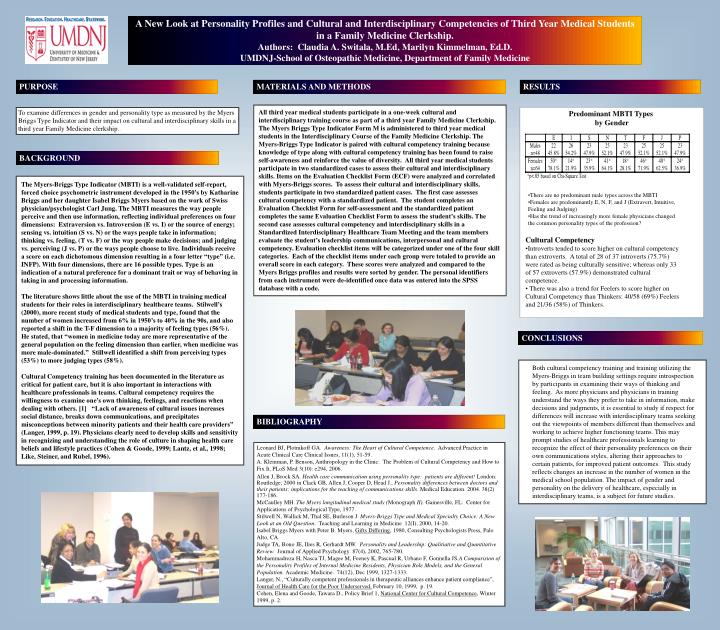
MATERIALS AND METHODS All third year medical students participate in a one-week cultural and interdisciplinary training course as part of a third year Family Medicine Clerkship. The Myers Briggs Type Indicator Form M is administered to third year medical students in the Interdisciplinary Course of the Family Medicine Clerkship. The Myers-Briggs Type Indicator is paired with cultural competency training because knowledge of type along with cultural competency training has been found to raise self-awareness and reinforce the value of diversity. All third year medical students participate in two standardized cases to assess their cultural and interdisciplinary skills. Items on the Evaluation Checklist Form (ECF) were analyzed and correlated with Myers-Briggs scores. To assess their cultural and interdisciplinary skills, students participate in two standardized patient cases. The first case assesses cultural competency with a standardized patient. The student completes an Evaluation Checklist Form for self-assessment and the standardized patient completes the same Evaluation Checklist Form to assess the student’s skills. The second case assesses cultural competency and interdisciplinary skills in a Standardized Interdisciplinary Healthcare Team Meeting and the team members evaluate the student’s leadership communications, interpersonal and cultural competency. Evaluation checklist items will be categorized under one of the four skill categories. Each of the checklist items under each group were totaled to provide an overall score in each category. These scores were analyzed and compared to the Myers Briggs profiles and results were sorted by gender. The personal identifiers from each instrument were de-identified once data was entered into the SPSS database with a code. BIBLIOGRAPHY Leonard BJ, Plotnikoff GA. Awareness: The Heart of Cultural Competence. Advanced Practice in Acute Clinical Care Clinical Issues, 11(1), 51-59. A. Kleinman, P. Benson, Anthropology in the Clinic: The Problem of Cultural Competency and How to Fix It, PLoS Med 3(10): e294, 2006. Allen J, Brock SA. Health care communication using personality type: patients are different! London: Routledge; 2000 in Clack GB, Allen J, Cooper D, Head J., Personality differences between doctors and their patients: implications for the teaching of communications skills. Medical Education. 2004. 38(2) 177-186. McCaulley MH. The Myers longitudinal medical study (Monograph II). Gainesville, FL: Center for Applications of Psychological Type, 1977. Stilwell N, Wallick M, Thal SE, Burleson J. Myers-Briggs Type and Medical Specialty Choice: A New Look at an Old Question. Teaching and Learning in Medicine 12(I), 2000, 14-20. Isabel Briggs Myers with Peter B. Myers, Gifts Differing, 1980, Consulting Psychologists Press, Palo Alto, CA. Judge TA, Bono JE, Ilies R, Gerhardt MW. Personality and Leadership: Qualitiative and Quantitative Review. Journal of Applied Psychology 87(4), 2002, 765-780. Mohammadreza H, Nasca TJ, Magee M, Feeney K, Pascual R, Urbano F, Gonnella JS.A Comparision of the Personality Profiles of Internal Medicine Residents, Physician Role Models, and the General Population. Academic Medicine. 74(12), Dec 1999, 1327-1333. Langer, N., “Culturally competent professionals in therapeutic alliances enhance patient compliance”, Journal of Health Care for the Poor Underserved, February 10, 1999, p. 19. Cohen, Elena and Goode, Tawara D., Policy Brief 1, National Center for Cultural Competence, Winter 1999, p. 2. A New Look at Personality Profiles and Cultural and Interdisciplinary Competencies of Third Year Medical Students in a Family Medicine Clerkship. Authors: Claudia A. Switala, M.Ed, Marilyn Kimmelman, Ed.D. UMDNJ-School of Osteopathic Medicine, Department of Family Medicine PURPOSE RESULTS To examine differences in gender and personality type as measured by the Myers Briggs Type Indicator and their impact on cultural and interdisciplinary skills in a third year Family Medicine clerkship.. Predominant MBTI Types by Gender BACKGROUND The Myers-Briggs Type Indicator (MBTI) is a well-validated self-report, forced choice psychometric instrument developed in the 1950’s by Katharine Briggs and her daughter Isabel Briggs Myers based on the work of Swiss physician/psychologist Carl Jung. The MBTI measures the way people perceive and then use information, reflecting individual preferences on four dimensions: Extraversion vs. Introversion (E vs. I) or the source of energy; sensing vs. intuition (S vs. N) or the ways people take in information; thinking vs. feeling, (T vs. F) or the way people make decisions; and judging vs. perceiving (J vs. P) or the ways people choose to live. Individuals receive a score on each dichotomous dimension resulting in a four letter “type” (i.e. INFP). With four dimensions, there are 16 possible types. Type is an indication of a natural preference for a dominant trait or way of behaving in taking in and processing information. The literature shows little about the use of the MBTI in training medical students for their roles in interdisciplinary healthcare teams. Stilwell’s (2000), more recent study of medical students and type, found that the number of women increased from 6% in 1950’s to 40% in the 90s, and also reported a shift in the T-F dimension to a majority of feeling types (56%). He stated, that “women in medicine today are more representative of the general population on the feeling dimension than earlier, when medicine was more male-dominated.” Stillwell identified a shift from perceiving types (53%) to more judging types (58%). Cultural Competency training has been documented in the literature as critical for patient care, but it is also important in interactions with healthcare professionals in teams. Cultural competency requires the willingness to examine one’s own thinking, feelings, and reactions when dealing with others. [1] “Lack of awareness of cultural issues increases social distance, breaks down communications, and precipitates misconceptions between minority patients and their health care providers” (Langer, 1999, p. 19). Physicians clearly need to develop skills and sensitivity in recognizing and understanding the role of culture in shaping health care beliefs and lifestyle practices (Cohen & Goode, 1999; Lantz, et al., 1998; Like, Steiner, and Rubel, 1996). • There are no predominant male types across the MBTI • Females are predominantly E, N, F, and J (Extravert, Intuitive, Feeling and Judging) • Has the trend of increasingly more female physicians changed the common personality types of the profession? • Cultural Competency • Introverts tended to score higher on cultural competency than extroverts. A total of 28 of 37 introverts (75.7%) were rated as being culturally sensitive; whereas only 33 of 57 extroverts (57.9%) demonstrated cultural competence. • There was also a trend for Feelers to score higher on Cultural Competency than Thinkers: 40/58 (69%) Feelers and 21/36 (58%) of Thinkers. CONCLUSIONS • Both cultural competency training and training utilizing the Myers-Briggs in team building settings require introspection by participants in examining their ways of thinking and feeling. As more physicians and physicians in training understand the ways they prefer to take in information, make decisions and judgments, it is essential to study if respect for differences will increase with interdisciplinary teams seeking out the viewpoints of members different than themselves and working to achieve higher functioning teams. This may prompt studies of healthcare professionals learning to recognize the effect of their personality preferences on their own communications styles, altering their approaches to certain patients, for improved patient outcomes. This study reflects changes an increase in the number of women in the medical school population. The impact of gender and personality on the delivery of healthcare, especially in interdisciplinary teams, is a subject for future studies.