Download
1 / 45
470 likes | 1.64k Views
0.7-2% of population per year seek medical attention for shoulder complaints (Roddey 2002)RTC tears become more common after 40 years of age (Boissonnault 2007)Partial thickness tears peak between ages 50-60 (Boissonnault 2007)Full thickness tears peak after age 60 (Boissonnault 2007)Five to forty percent of population over age 60 has evidence of full thickness rotator cuff tear (Boissonnault 2007).

E N D
1. Alison Deichert PT, DPT
September 17, 2011
Midwest Student Conclave Exercise PROGRESSION and rehabilitation considerations following rotator cuff repair
2. 0.7-2% of population per year seek medical attention for shoulder complaints (Roddey 2002)
RTC tears become more common after 40 years of age (Boissonnault 2007)
Partial thickness tears peak between ages 50-60 (Boissonnault 2007)
Full thickness tears peak after age 60 (Boissonnault 2007)
Five to forty percent of population over age 60 has evidence of full thickness rotator cuff tear (Boissonnault 2007)
PREVALANCE OF ROTATOR CUFF INJURIES Percentage even higher for athletesPercentage even higher for athletes
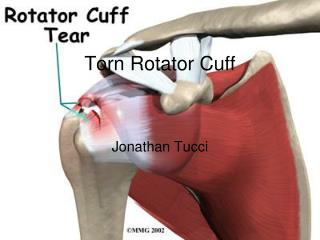
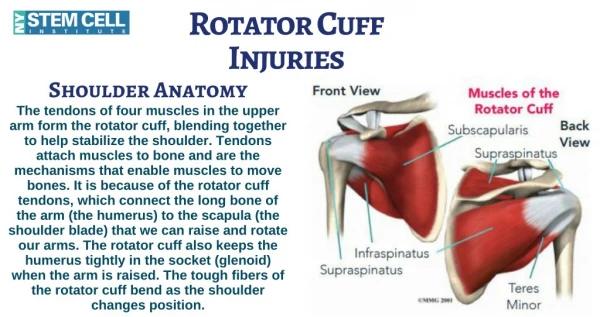
3. Rotator cuff musculature
4. Dynamic stabilizer of rotator cuff in multiple positions (Reinold 2009)
Balances force couples about the glenohumeral joint (Lo 2003)
Helps to resist superior translation of humeral head, to center the humeral head in the glenoid
Inman (1994) discussed coronal plane force couple between deltoid and posterior cuff (infraspinatus, teres minor, and subscapularis)
Transverse plane force couple is subscapularis anteriorly balanced against infraspinatus and teres minor (Lo 2003) Rotator cuff FUNCTION If infraspinatus and teres minor torn then will not create large enough moment to balance posterior cuff and humeral head will translate superior and anteriorly. Goal with sx is to return normal force alignment
Rotator cuff counteracts shearing force generated by deltoid-creates compression of HH in glenoidIf infraspinatus and teres minor torn then will not create large enough moment to balance posterior cuff and humeral head will translate superior and anteriorly. Goal with sx is to return normal force alignment
Rotator cuff counteracts shearing force generated by deltoid-creates compression of HH in glenoid
5. Has greatest ROM of any joint in body (Wilk 1997)
Articular surface of glenoid is pear shaped
Glenoid is much smaller then humeral head
During normal motion only 25-30% of the humeral head is actually in contact with glenoid (Wilk 1997) GLENOHUMERAL JOINT Inherently unstable-most commonly dislocated joint-sacrifices stability for mobility
Surface area of humeral head is 3-4x that of glenoid
Main function of the glenohumeral joint-to position the hand for function
Golf ball on a teeInherently unstable-most commonly dislocated joint-sacrifices stability for mobility
Surface area of humeral head is 3-4x that of glenoid
Main function of the glenohumeral joint-to position the hand for function
Golf ball on a tee
6. Glenohumeral joint
7. ROLE IN STABILITY: provide stable base of support for glenohumeral joint muscles to function from (Wilk 1997)
Maintains a dynamic and consistent length tension relationship for shoulder girdle
Correlation exists between weak scapular muscles and MDI (Wilk 1997) SCAPULOTHORACIC MUSCULATURE
8. EDUCATE YOUR PATIENT:
Sling wear, wound management, healing times, safety
PROTECT THE REPAIR
IMPROVE DYNAMIC STABILIZATION
DECREASE PAIN
PROMOTE HEALING
RESTORE PASSIVE MOTION
IMPROVE MUSCULAR STRENGTH AND BALANCE
(Ghodadra 2009 and Wilk 2009) REHABILITATION GOALS FOLLOWING ROTATOR CUFF REPAIR 12 weeks to obtain adequate pull out strength of the repair12 weeks to obtain adequate pull out strength of the repair
9. OPEN
MINI-OPEN DELTOID SPLITTING TECHNIQUE
ARTHROSCOPIC
TYPES OF ROTATOR CUFF REPAIR
10. First rotator cuff repair was done in 1911 by Dr. Codman using open technique (Ghodadra 2009)
5 Fundamentals of Repair according to Neer in 1972 include:
Meticulous repair of deltoid origin
Subacromial decompression
Surgical releases as necessary to mobilize tissue
Secure fixation of tendon to tuberosity
Closely supervised rehab with early PROM
(Ghodadra 2009)
OPEN ROTATOR CUFF REPAIR
11. 3-6 inch incision made over anterior superior aspect of the shoulder
Deltoid taken off acromion and split for 3-5 centimeters
Deltoid must be reattached following repair OPEN ROTATOR CUFF REPAIR PROCEDURES
12. PROS:
Allows for easier visualization of tissue
Good for repairing large or massive tears
Complication rate of 10.5% (Mansat 1997)
Demonstrates high rates of pain relief, functional improvement, improved ROM, and overall patient satisfaction in various studies
CONS
Increased postoperative pain
Deltoid takedown
Infection risk/hospitalization (Lindenfeld 2009)
Slower rehab-longer period of protection and/or immobilization following deltoid takedown and repair (Ghodadra 2009) OPEN ROTATOR CUFF PROS/CONS
13. Levy developed in 1994 to avoid deltoid issues
Uses arthroscope to perform subacromial decompression and then opens up to do rotator cuff repair
Uses 3-5 centimeter incision along deltoid along with other portals
MINI-DELTOID SPLITTING TECHNIQUE
14. PROS:
Preserves deltoid attachment
Less soft tissue dissection
Provides results similar to open repair
Decreased pain
Complication rate of 8.8% (Curtis 1992)
Quicker rehabilitation protocol
CONS:
Limited access to joint
Risk of deltoid detachment
Can be difficult if tear is to large (Lindenfeld 2009)
Need for extensive surgical experience (Ellenbecker 2006) MINi-DELTOID SPLITTING PROS/CONS
15. Small incisions of 7-8 millimeters
Use anterior portal lateral to coracoid of 5-6 mm. Cannula enters here into glenohumeral joint (Ghodadra 2009)
Lateral portal with possible superior lateral accessory portal also.
1 centimeter incision at posterior portal Arthroscopic repair pROCEDURES
16. PROS:
Lower risk of complications
Improved cosmesis
Decreased pain post surgery
Avoids deltoid detachment
Earlier return to work and sport (Shinners 2002)
CONS:
Lack of long term outcome data
Technical difficulty
Fixation method questions
Brislin noted complication rate of 10.6% (2007) Arthroscopic pros/cons
17. Yourpracticeonline.com.au/rotator-cuff-tear-3dvideo.html
You Tube has several great videos to choose from ARTHROSCOPIC VIDEO
18. SIZE OF TEAR
Small tear- less then 1 cm
Medium tear 1-3 cm
Large tear 3-5 cm
Massive tear > 5 cm
Full thickness vs. partial tear:
Partial can occur on bursal side from subacromial impingement or undersurface from tensile loads and GHJ instability.(Ellenbecker 2006)
Full thickness involve top to bottom of tendon. Often occur in supraspinatus (Ellenbecker 2006)
OTHER REHABILITATION CONSIDERATIONS-TEAR SIZE If 2 tendons involved will lead to altered stress patterns on GHJ joint but one tendon lesion did not.
Tear < 50% debride, > 50% repair Dr. Hasan
Multiple studies show that have worse outcome and highest rate of retear with massive tearsIf 2 tendons involved will lead to altered stress patterns on GHJ joint but one tendon lesion did not.
Tear < 50% debride, > 50% repair Dr. Hasan
Multiple studies show that have worse outcome and highest rate of retear with massive tears
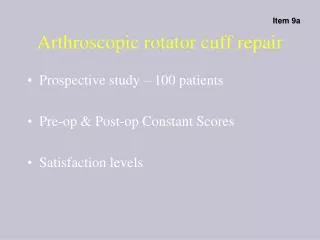
19. Small Rotator cuff tear
Source: http://www.bjc-houston.com Small rotator cuff TEAR
20. MEDIUM ROTATOR CUFF TEAR
21. Large rotator cuff tear
22. TISSUE QUALITY:
Look at quality of tendon, muscle and bone
Thin tissue, soft bone, fatty infiltrate of musculature will all effect rehab speed, (Ghodadra 2009)
TYPE OF FIXATION
Single row anchors vs. double row
Multiple studies show double row repair is stronger
OTHER REHABILITATION CONSIDERATIONS Smoking, DM, osteoporosis, previous cancer can all also affect tissue qualitySmoking, DM, osteoporosis, previous cancer can all also affect tissue quality
23. LOCATION OF TEAR- which tendons are involved?
SURROUNDING TISSUE QUALITY-what do the other RTC muscles look like?
MECHANISM OF FAILURE-
Traumatic (3-5%)
Gradual wear (95%)
How long tear has been present may affect rehab
PATIENT VARIABLES-
age, activities, general health, work status
(Ghodadra 2009)
OTHER REHABILITATION CONSIDERATIONS Supraspinatus only typically has smaller sized tears. Posterior shoulder require greater protection. Subscap tear rare-more often with anterior dislocation-more limited ROMSupraspinatus only typically has smaller sized tears. Posterior shoulder require greater protection. Subscap tear rare-more often with anterior dislocation-more limited ROM
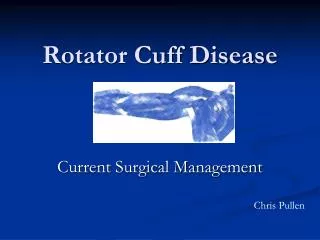
24. TYPE OF TEAR- 3 main types
Crescent tear-doesn�t retract far and can be fixed directly to the greater tuberosity.
Source: Http://www.jaaos.org
TYPES OF TEARS-Crescent shaped
25. TYPE OF TEAR- 3 main types
U Shaped Tear-Greatest area of tear is longitudinally to the bone. Repair first through margin convergence and then fix the crescent tear to the bone. (Ellenbecker 2006) Source: Http://www.jaaos.org
Types of tears-u shaped
26. L shaped tear- one of the leaves (usually posterior) is more mobile and can be brought to the other leaf (Ghodara 2009 and Wilk 1997)
TYPES OF TEARS- L SHAPED
27. ACCESS TO CARE
SURGEON�S PHILOSOPHY
CONSERVATIVE VS. AGGRESSIVE
(Ghodadra 2009)
OTHER REHABILITATION CONSIDERATIONS
28. Vary based on previously discussed factors
Vary depending on SIZE OF TEAR
Each surgeon will have their own preferences!!
Overall philosophy of progression is fairly similar but the TIMING of progressions can be different
ReHABilitation PROTOCOLS
29. Initial protection phase- 0-6 weeks
Active Range of motion- 4-6 weeks
Strengthening- 8-16 weeks
Return to sport- 16 weeks + BASIC GUIDELINES
30. Immediate PROM
Flexion may be limited to 90-120 degrees initially
ER/IR at 45 degrees abduction to 25-30 degrees initially
Elbow, wrist, hand ROM
ICE 4-6x/day for 15-20 minutes
Patient education KEY!!
PENDULUMS:
Long et. al studied healthy subjects and found that large correct and large incorrect pendulums both produce maximum voluntary isometric contraction (MVIC) > 15% of supraspinatus and infraspinatus. (2010).
INITIAL REHAB DAY 1
31. Continue with PROM to tolerance per guidelines
May begin Neuromuscular Stimulation
Reinold performed study that showed a 22% peak force production in patients that received NMES vs. those whose didn't (2008).
Utilized Empi 300 PV to patient�s tolerance at 10.5�7.1 days postop
Start rhythmic stabilization ER/IR at 45 degrees abduction REHAB WEEK 1-2 Positioned at 45 degrees abduction, neutral rotation at 15 degrees horizontal adduction with bolster under distal humerus
Pads on infraspinatus
Positioned at 45 degrees abduction, neutral rotation at 15 degrees horizontal adduction with bolster under distal humerus
Pads on infraspinatus
32. Continue with PROM progressing as indicated
Joint mobs begin weeks 3-4
Begin scapulothoracic exercises/scapular clock
Smith et. Al (2006) showed that scapular depression and protraction produced MVC < 20% of the supraspinatus, infraspinatus, and deltoid
Can do these early in rehab without harm
Isometrics-SUBMAXIMAL/PAIN FREE
Flex/ER/IR Rehab week 2-4
33. Need to have FULL PROM by week 4-6
Would like to see dynamic humeral head control by 6 weeks
Goals of first phase of rehab include restoring ROM, decreasing pain and creating baseline proprioception and kinesthetic awareness (Wilk 2009) Early goals
34. Progressing to AROM Begin with ROM in supine or sidelying (Ellenbecker 2006)
DO NOT work through a shrug sign!!
Begin basic closed chain exercises
Closed chain exercises increases shoulder proprioception, stability and muscle coactivation
Start with prayer and quadruped exercises (Uhl 2003)
allows for arm to be used in a functional length tension arc with minimal gravitational effects (Ellenbecker)
Uhl et. Al demonstrated that these positions are appropriate for earlier rehab phases.
EMG showed low activity in all tested musculature-supraspinatus, infraspinatus, anterior and posterior deltoid, and pec major
allows for arm to be used in a functional length tension arc with minimal gravitational effects (Ellenbecker)
Uhl et. Al demonstrated that these positions are appropriate for earlier rehab phases.
EMG showed low activity in all tested musculature-supraspinatus, infraspinatus, anterior and posterior deltoid, and pec major
35. Side lying external rotation (SLER)
Reinold demonstrated that SLER produced the highest combined EMG signal for infra and supraspinatus (62 and 67%)
Showed increased EMG activity with towel roll placed under arm
20-25% increase in EMG signal with use of towel roll vs. not
PNF DYNAMIC STABILITY-TOTAL ARM STRENGTH
36. Full can exercise-best to isolate supraspinatus
Reinold (2007)looked at full can, empty can and prone full can exercise.
All 3 produced 62-67% of MVIC of SUPRASPINATUS. Demonstrated increased posterior and middle deltoid activity with EMPTY and PRONE FULL can.
Prone Rowing- weighted or manually resisted
Best exercise per EMG for middle trap (Reinold 2009)
Dynamic stability total arm strength
37. Isotonic scapular strengthening exercises
PRONE EXTENSION- activates middle and lower trap before the posterior deltoid. Activates middle and lower trap before the upper trap (DeMey 2009). Produced 3rd highest EMG activity in rhomboids and levator per Reinold 2009
PRONE HORIZONTAL ABDUCTION WITH ER- same activation pattern as prone extension per DeMey . Demonstrated 3rd highest upper trap, 2nd highest middle trap, rhomboid, and levator EMG activity per Reinold 2009.
PRONE FULL CAN- Highest EMG activity for lower trapezius per Reinold and Ekstrom (97% EMG) and 2nd highest amount of EMG activity for supraspinatus
PRONE OVERHEAD ARM RAISE � Ekstrom demonstrated to produce the highest EMG for mid trap (101%) DYNAMIC STABILITY-total arm strength
38. Supine punch at 90 degrees and 120 degrees-
Ekstrom demonstrated 62% MVIC of serratus, 3rd highest EMG activation of serratus per Reinold
Dynamic Hug
Ekstrom demonstrated 53% of serratus activity with this exercise while Reinold rated it the 2nd best exercise for serratus
Diagonal shoulder flexion, horizontal flexion and ER
Ekstrom demonstrated 100% MVIC of serratus with this activity and is easier for patients with impingement to do.
Theraband exercises DYNAMIC STABILIZATION-TOTAL ARM STRENGTH
39. Tripod and pointer exercise-moderate demand on posterior deltoid and infraspinatus (Uhl 2007)
Wall pushups with plus-
Best exercise for serratus per EMG (Reinold 2009)
Wall stabilization with ball
Rhythmic stabilization in plank and/or pushup position
DYNAMIC STABILIzation-total arm strength
40. Initiate pushup position
Demonstrates higher demands on infraspintus, moderate anterior deltoid and pec major activity, while posterior deltoid decreases to low level of activity per Uhl
Wall dribbles
Body blade
Resisted PNF while sitting on ball
Planks with theraband/unstable surfaces
Pushup stepups
Rebounder exercises when allowed
Ball flip exercise
(Wilk and Payne 2009) Return to activity
41. Focus on using light weights throughout the rehab program
Remeasure daily in the passive ROM phase
Avoid biceps irritation
Develop an appropriate muscle balance with good ER/IR ratio with scapular strength
Final thoughts
42. Boissonnault WG, Badke MB, Wooden MJ, Ekedahl S, Fly K. Patient outcome following rehabilitation for rotator cuff repair surgery: the impact of selected comorbidities. J Orthop Sports Phys Ther. 2007;37(6): 31.2-319.
Brislin KJ, Field LD, Savoie FH. Complications after arthroscopic rotator cuff repair. Arthroscopy. 2007; 23(2): 124-128.
Curtis AS, Snyder SJ, Del Pizzo W, Friedman MH, Ferkel RD, Karzel RP. Complications in arthroscopic shoulder surgery. Arthroscopy. 1992; 8:395.
De Mey K, Cagnie B, Van De Velde A, Danneels L, Cools AM. Trapezius muscle timing during selected shoulder rehabilitation exercises. J Orthop Sports Phys Ther. 2009: 39(10): 743-752.
References
43. Ekstrom RA, Donatelli RA, Soderberg GL. Surface Electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther. 2003; 33: 247-258.
Ellenbecker TS, Balle DS, Kibler WB. Rehabilitation after mini open and arthroscopic repair of RTC. Postsurgical orthopedic sports rehabilitation of knee and shoulder. Manske RC. 665-681. Mosby Elsevier. 2006 St. Louis MO.
Ghodadra NS, Provencher MT, Verma NN, Wilk KE, Romeo AA. Open, Mini open and all-arthroscopic rotator cuff repair surgery: indications and implications for rehabilitation. J Orthop Sports Phys Ther. 2009: 39(2): 81-89
Hasan SS. (May 2009) Treatment of Partial Thickness Rotator Cuff Tears. Lecture Presentation at the 24th annual Advances on the Knee and Shoulder conference. Hilton Head South Carolina.
Inman VT, Saunders JR, Abbott JC. Observations on the function of the shoulder joint. J Bone Joint Surg. 1994: 26; 1-30. References
44. Lindenfeld TN. (May 2009). Open rotator cuff repair and managing the irreparable tear. Lecture presentation at the 24th annual Advances on the knee and shoulder conference. Hilton Head South Carolina.
Lo IKY, Burkhart SS. Spotlight on surgical techniques-current concepts in arthroscopic rotator cuff repair. Am J Sports Med. 2003: 31(2): 308-324
Long et. Al. Activation of the shoulder musculature during pendulum exercises and light activities. J Orthop Sports Phys Ther. 2010; 40(4): 230-237.
Mansat P, Cofield FH, Kersten TE, Rowland Cm. Complications of rotator cuff repair. Orthop Clin North Am. 1997; 28: 205-213.
Reinold RM, Escamilla R, Wilk KE. Current concepts in the scientific and clinical rationale behind exercises for glenohumeral and scapulothoracic musculature. J Orthop Sports Phys Ther. 2009; 39(2): 105-117.
Reinold RM, et al. Electromyographic analysis of the supraspinatus and deltoid muscles during three common rehabilitation exercises. J Athl Training. 2007; 42(4): 464-469.
References
45. Reinold RM, Macrina LC, Wilk KE, Duga JR, Cain EL, Andrews JA. The effect of neuromuscular electrical stimulation of the infraspinatus on shoulder external rotation force production after rotator cuff repair surgery. Am J Sports Med. 2008; 36: 2317-2320.
Roddey TS, Olson SL, Gartsman GM, Hanten WP, Cook KF. A randomized controlled trial comparing 2 instructional approaches to home exercise instruction following arthroscopic full-thickness rotator cuff repair surgery. J Orthop Sports Phys Ther. 2002; 32:548-559.
Shinners TJ, Noordsij PG, Orwin JF. Arthroscopically assisted mini-open rotator cuff repair. Arthroscopy. 2002; 18(1): 21-26.
Smith et. Al. Electromyographic activity in the immobilized shoulder girdle musculature during scapulothoracic exercises. Arch Med Phys Rehabil. 2006; 87: 923-927.
Uhl TL, Carver TL, Mattacola CG, Mair SD, Nitz AL. Shoulder musculature activation during upper extremity weight bearing exercise. J Orthop Sports Phys Ther. 2003; 33: 109-117. references
46. Wilk KE, Arrigo CA, Andrews JA. Current concepts: the stabilizing structures of the glenohumeral joint. J Orthop Sports Phys Ther. 1997; 25(6): 364-379
Wilk KE. (May 2009). Rehabilitation following rotator cuff tear. Lecture presentation at 24th annual Advances on the knee and shoulder conference. Hilton Head South Carolina.
Wilk KE, Payne RM. Dynamic stability vs. mobility: which exercises are best for shoulder girdle musculature. Lecture and lab presentation at 24th annual Advances on the knee and shoulder conference. Hilton Head South Carolina. references