Download
1 / 33
360 likes | 976 Views
Sports Physiotherapy. Group presentation Topic 2 Chan Hung Kai #9 Chan Yu Kai #19 Chow Hau Tak #39 Lue Jacky # 91. Case Introduction. Mary is a player of Hong Kong Basketball Team She twisted her (L) knee while landing from a rebound during competition 3 months ago

E N D
Sports Physiotherapy Group presentation Topic 2 Chan Hung Kai #9 Chan Yu Kai #19 Chow Hau Tak #39 Lue Jacky # 91
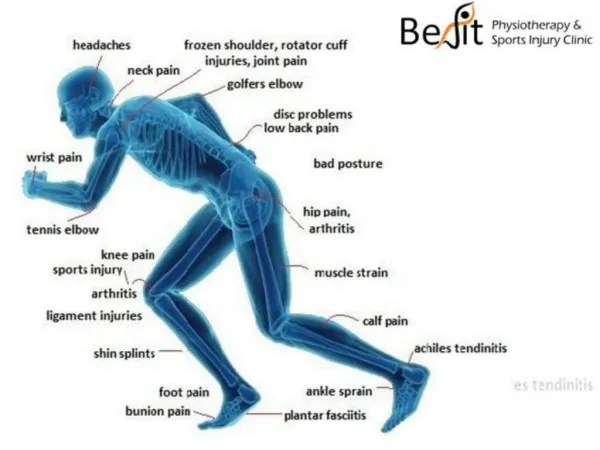
Case Introduction • Mary is a player of Hong Kong Basketball Team • She twisted her (L) knee while landing from a rebound during competition 3 months ago • Suffered from a grade II ACL injury • How would you prepare Mary for a safety return to her sport as a PT?
Outlines of Presentation • Epidemiology • Risk factors for female athletes • Special demand on ACL for female basketball player • Rehabilitation training • Female athletes physical conditioning • Psychological preparation • Q and A session
Epidemiology of ACL for Female • Female athletes have a significantly increased risk of ACL injuries than male counterparts in soccer and basketball almost universal in all levels of play (Ireland , 1999) • In inter-college basketball, female were 6.19 as likely to sustain ACL injury than males. (Malone et al 1993 in Emerson R.J., 1993)
Risk factors for ACL in Female • Hamstring-to-Quads ratio significantly higher in male athletes (P<0.04) (Anderson et al, 2001) • Women are slower in generating peak Hamstring torque (Hewett et al, 1999, Winter & Brookes , 1991) • HQ ratio <50% (P<0.05), Quadriceps are dominant in woman both in terms of strength and firing pattern. (Hewett et al, 1999)
Risk factors for ACL in Female • Smaller ACL in Woman (after adjustment for weight) and it probably does not compensate for its decreased stiffness and strength, P=0.03 (Anderson et al, 2001) • Estrogen level changes metabolism of ACL which can reduce the ACL strength, P<0.001 (Liu et al, 1997) Also demonstrated in Heitz et al, 1999) • Increased Q-angle places the knees in a more valgus or unstable position (Boden et al, 2000, Heitz et al, 1999)
Implications of ACL deficiency in female basketball player • ACL deficiency : (Swenson et al, 1995) • Increase anterior tibial translation • Increase varus and valgus angulation and tibial rotation • Decrease proprioception of the knee • Basketball skills that demands the most from ACL: (Ireland, 1999) • Landing from jumping • Pivoting and Cutting
Landing from Jumping • Landing from jumping • Mainly in Jump shot, • Lay up • Guarding (block shot) • Rebounding
Implication of ACL deficiency on Landing • Landing forces from jumping after guarding or shooting are high (Hewett et al, 1999) • ACL act as the primary restrainer to withstand those shocks during landing and prevent tibial translation • ACL deficiency would result in the instability and concomitant injuries on the knee during landing
Pivoting and Cutting • Pivoting and cutting: • Mainly for dribbling, • Defense, • Post-up
Implication of ACL deficiency on Pivoting and Cutting • During pivoting and cutting (Heitz et al, 1999) • The player needs to decelerate and change direction • the lower leg is fixed and rotated • Angulation force is placed on the knee • ACL deficiency would result in instability in pivoting and cutting
Rehabilitation training (Fitzgerald et al, 2000a) • Muscle strengthening exercise • Cardiovascular endurance training • Agility and sport-specific skill training • Perturbation training
Muscle strengthening exercise (Fitzgerald et al, 2000a) • Strengthen the quadriceps and hamstring • Exercise include: 1. Resisted leg curls 2. Leg press 3. Squat
Cardiovascular training (Fitzgerald et al, 2000a) • Should be related to the patient’s sport • Should be proceed and progress when patient does not complain pain or swelling
Agility and sport specific skill training (Fitzgerald et al, 2000a) • Agility training includes: 1. Side slides 2. Carioca Promote quick changes in direction and lateral movement 3. Shuttle run 4. Cutting and spinning Promote quick starting • Initiated at half speed and progress to full-speed
Sport-specific training (Fitzgerald et al, 2000a) • Pre-requisite: Can perform full-speed agility training No pain No swelling No hesitation • For basketball players: Dribbling Jump shot Lay-up
Sport-specific training (Fitzgerald et al, 2000a) • Progression: 1. Without opponents 2. One-to-one 3. Full practice
Perturbation training (Fitzgerald et al, 2000a) • Aim: induce compensatory alteration in muscle activity patterns • Applied with the patient stand on tilt broad or roller broad • Translational and rotational perturbation • Similar to rhythmic stabilization
Efficacy of Perturbation training (Fitzgerald et al, 2000b) • For the standard treatment group: 7 of 14 subjects have unsuccessful rehabilitation • For the perturbation group: 1 of 12 subjects have unsuccessful rehabilitation The successful rate for the perturbation group is 5 times of the standard treatment group
Female specific Training • Tend to be quadriceps dominant (Laura 1996)Focus on hamstring and gastrocnemius strengthening (Medvecky 2000), eg. Jumping ex : improve technique & strength (Hewett et al, 1999) but no relationship is shown between strength & mm reaction time (Wojtys et al 1996)Agility Training> isokinetic & isotonic training (Wojtys et al 1996) • Smaller ACL, increased Q-angle and estrogen levelNon-changeable
Jumping Programs (Hewett et al 1999) • Decrease the peak landing force • Decrease abduction and adduction moments during landing (those are less stable positions) • Correct the imbalance and bring the ratio of hamstring to quadriceps isokinetic strength in female athletes to the same level of male athletes • Improve coactivation of hamstring mm in athletes with quadricep-to-hamstring strength imbalance after hamstring mm training exercises. • Improvements in technique and strength
Female specific Training(Christensen 1993) • Lower overall strength • Large stores of body fat • Lower VO2 max • Lower anaerobic power • Similar response of physical training between male and female (Drinkwater 1984 in Christensen 1993)
Other Considerations • Female Athlete Triad (FAT)(Otis 1997; Burrows 2000) • Disordered eating-Habits, sport features -Stress • Amenorrhea -Over-training-Insufficient body fat and body weight-Insufficient diet to meet energy requirement-Psychological and physical stress • Osteoporosis-Stress fracture
Other Considerations • Preventions of FAT(Burrows 2000) • Training modification • Education to the athletes and also the coaches • Change in behavior esp. on nutrition
Psychological Methods to Overcome fear. • Mental training: • General Relaxation training, which increases body awareness and decreases fear. • Mental rehearsal, to imagine the movement and the sport situation. • Self-talk, use of assertive statement to gain confidence
Other Considerations that reduce fear • Reassurance of the environment and her physical condition • Education on how to jump and land safely • Use of knee brace to gain psychological reassurance. • According to the study of Colville et al, (1986) Lenox Hill brace, significantly reduce symptoms of instability and giving way and athletic performance improved by 69% during brace.
Overcome fear through Training • Start slowly by jumping and landing on level ground. • Progress by jumping from a step • Increase the height of the step • Practice jump shoot, rebounding and lay up. • Jump on a bouncer (unstable surface). • Progress with single leg jump. • Plyometric drill.
Conclusion • Female is prone to more ACL injury • Training should focus on • General physical training • Sport-specific skills • Gender aspect • Psychological aspect
References 1 • Anderson AF., Dome DC., Gautam S., Awh MH., Rennirt GW. (2001). Correlation of anthropometric measurements, strength, anterior cruciate ligament size, and intercondylar notch characteristics to sex differences in anterior cruciate ligament… AJSM. 29(1):58-66. • Boden BP., Griffin LY., Garrett WE. (2000). Etiology and Prevention of noncontact ACL injury. The Physician and Sportsmedicine. 53. • Burrows M., Bird S. (2000): The physiology of the highly trained female endurance runner.[Review] Sports Med. 30(4): 281-300 • Christensen C.L.:Women in sport : issues and controversies. Chapter 11.Newbury Park : Sage Publications, c1993 • Fitzgerald GK, Axe MJ, Snyder-Mackler L.(2000a): Proposed practice guidelines for nonoperative anterior cruciate ligament rehabilitation of physically active individuals. JOSPT. 30(4): 194-203 • Fitzgerald GK, Axe MJ, Snyder-Mackler L.(2000b): The efficacy of perturbation training in nonoperative anterior cruciate ligament rehabilitation programs for physically active individuals. Physical Therapy 80(2): 128-139 • Heil J. (1993). Psychology of Sport Injury. Human Kinetics. Canada:152-153. • Heitz NA., Eisenman PA., Beck CL., Walker JA. (1999). Hormonal changes throughout the menstrual cycle and increased anterior cruciate ligament laxity in females. Journal of Athletic Training. 34(2):144-9. Hewett TE, Lindenfeld TN, Riccobene JV et al. (1999). The effect of neuromuscular training on the inccidence of knee injury in female athletes: a prospective study. AJSM 27(6):699-706.
References 2 • Holloway JB, Baechle T (1990): Strength training for female athletes. A review of selected aspects. Sports Medicine 9(4): 216-228 • Ireland ML. (1999). Anterior cruciate ligament injury in female athletes: Epidemiology. Journal of Athletic Training. 34(2):150-4. • Laura JH, Edward MW. (1996): Neuromuscular performance characteristics in elite female athletes. AJSM 24(4): 427 • Liu SH., Al-Shaikh RA., Panossian V., Finerman GAM, Lane JM. (1997). Estrogen affects the cellular metabolism of the anterior cruciate ligament:A potential explanation for female athletic injury. AJSM. 25(5):704-9. • Medvecky MJ, Bosco J, Shermen OH. (2000): Gender disparity of anterior cruciate ligament injury. Etiological theories in female athlete. Bulletin of Hospital for Joint Diseases. 59(4): 217-226. [Abstract] • Otis C.L., Drinkwater B., Johnson M. et al (1997 May) : American College of Sport Medicine position stand. The female athlete triad. Medicine & Science in Sport & Exercise. 19(5):i-ix • Swenson TM., Harner CD. (1995) Knee Ligament and Meniscal Injuries:Current concepts. Sports Medicine. 26(3):529-546. • Winter EM., Brookes FB. (1991). Electromechanical response times and muscle elasticity in men and women. Eur J Appl Physiol Occup Physiol. 63:124-128. • Wojtys EM, Huston LJ, Taylor PD & Bastian SD (1996). Neuromuscular adaptations in isokinetic, isotonic, and agility training programs. AJSM 24(2): 187-192