Download
1 / 51
550 likes | 959 Views
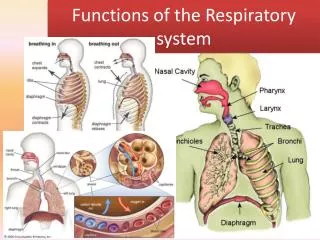
Five Functions of the Respiratory System. Provides extensive gas exchange surface area between air and circulating blood Moves air to and from exchange surfaces of lungs Protects respiratory surfaces from outside environment Produces sounds Participates in olfactory sense.

E N D
Five Functions of the Respiratory System • Provides extensive gas exchange surface area between air and circulating blood • Moves air to and from exchange surfaces of lungs • Protects respiratory surfaces from outside environment • Produces sounds • Participates in olfactory sense
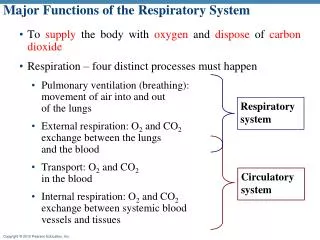
Major Functions of the Respiratory System • To supply the body with oxygen and dispose of carbon dioxide • Respiration – four distinct processes must happen • Pulmonary ventilation (breathing):movement of air into and outof the lungs • External respiration: O2 and CO2exchange between the lungsand the blood • Transport: O2 and CO2in the blood • Internal respiration: O2 and CO2exchange between systemic bloodvessels and tissues Respiratory system Circulatory system
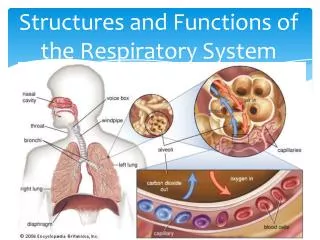
Respiratory System – conducting and respiratory zone • Consists of the respiratory and conducting zones • Respiratory zone: • Site of gas exchange • Consists of respiratory bronchioles, alveolar ducts, and alveoli • Conducting zone: • Conduits for air to reach the sites of gas exchange • Includes all other respiratory structures (e.g., nose, nasal cavity, pharynx, trachea) • Respiratory muscles – diaphragm and other muscles that promote ventilation
Respiratory System – conducting and respiratory zone • Conducting passageways carrying air to and from the alveoli • Upper respiratory passages filter and humidify incoming air • Lower passageways include delicate conduction passages and alveolar exchange surfaces • The conducting passageways of the respiratory system (nasal cavity, trachea, bronchi and bronchioles) are lined by ciliated pseudostratified columnar ET, which includes mucus-secreting goblet cells. • Because the passage of air depends on wide open passageways, the larger respiratory passages (trachea and bronchi) are supported by rings of cartilage. • The respiratory regions are lined with simple squamous ET
Function of the Nose • The only externally visible part of the respiratory system that functions by: • Providing an airway for respiration • Moistening and warming the entering air • Filtering inspired air and cleaning it of foreign matter • Serving as a resonating chamber for speech • Housing the olfactory receptors
Paranasal Sinuses • Sinuses in bones that surround the nasal cavity • Sinuses lighten the skull and help to warm and moisten the air http://sinusitis.upmc.com/Images/Sub/PhotoSinusitis.jpg
Larynx (Voice Box) • Attaches to the hyoid bone and opens into the laryngopharynx superiorly • Continuous with the trachea posteriorly • The functions of the larynx are: • Air passage • To act as a switching mechanism to route air and food into the proper channels • To function in voice production
Framework of the Larynx • Cartilages (hyaline) of the larynx • Shield-shaped anterosuperior thyroid cartilage with a midline laryngeal prominence (Adam’s apple) • Signet ring–shaped anteroinferior cricoid cartilage • Three pairs of small arytenoid, cuneiform, and corniculate cartilages • Epiglottis – elastic cartilage that covers the laryngeal inlet during swallowing • Glottis is the superior opening of the larynx. It is guarded by the epiglottis (cartilage)
Vocal Ligaments • Attach the arytenoid cartilages to the thyroid cartilage • Composed of elastic fibers that form mucosal folds called true vocal cords • The medial opening between them is the glottis • They vibrate to produce sound as air rushes up from the lungs • False vocal cords • Mucosal folds superior to the true vocal cords • Have no part in sound production
Voice Production • Speech: release of expired air while opening and closing the glottis • Pitch is determined by the length and tension of the vocal cords • Loudness depends upon the force of air • Chambers of pharynx, oral, nasal, and sinus cavities amplify and enhance sound quality • Sound is “shaped” into language by muscles of the pharynx, tongue, soft palate, and lips
Trachea • Flexible and mobile tube extending from the larynx into the mediastinum • Composed of three layers • Mucosa – ciliated pseudostratified columnar epithelium with goblet cells • Submucosa – connective tissue with mucous glands, lymph nodes • Adventitia – fibrous CT that contains C-shaped rings of hyaline cartilage
The primary bronchi • Trachea branches in the mediastinum into right and left primary bronchi • Bronchi enter the lungs at the hilus • Have C-shaped cartilaginous supporting rings
The bronchial tree • System of tubes formed from the primary bronchi and their branches • Primary bronchi branch into secondary or lobar bronchi • Secondary bronchus goes to each lobe of the lungs • Secondary bronchi branch into tertiary (segmental) bronchi • Both secondary and tertiary bronchi are covered by overlapping plates of cartilage and not rings • Cartilage in walls decrease and smooth muscle increase with branching
The Bronchi and Lobules of the Lung Figure 23.10a
The bronchioles • Branching of the bronchi that are 1 mm or less in diameter and lack cartilage. Bronchioles are surrounded by smooth muscle that allows the change of diameter. • Ultimately bronchioles branch into the final branch of the conducting division - terminal bronchioles with a diameter of 0.3-0.5 mm • Terminal bronchiole becomes respiratory bronchioles – the beginning of the respiratory division
Respiratory Zone • Defined by the presence of alveoli; begins as terminal bronchioles feed into respiratory bronchioles • Respiratory bronchioles lead to alveolar ducts, then to terminal clusters of alveolar sacs composed of alveoli • Approximately 300 million alveoli: • Account for most of the lungs’ volume • Provide tremendous surface area for gas exchange
Respiratory Membrane • This air-blood barrier is composed of: • Alveolar and capillary walls • Their fused basal laminas • Simple squamous ET (type I) – most of the cells in the alveolus wall and are part of the respiratory membrane (allow gas exchange) • Septal cells (type II ) – about 5% of the alveolar wall. The septal cells secret surfactant – a lipoprotein secretion that reduces the surface tension in the alveolus • Alveolar Macrophage (dust cells) - patrol epithelium and engulf foreign particles
Pleurae • Thin, double-layered serosa • Parietal pleura • Covers the thoracic wall and superior face of the diaphragm • Continues around heart and between lungs • Visceral, or pulmonary, pleura • Covers the external lung surface • Divides the thoracic cavity into three chambers • The central mediastinum • Two lateral compartments, each containing a lung
Breathing or pulmonary ventilation • A mechanical process that depends on volume changes in the thoracic cavity • Volume changes lead to pressure changes, which lead to the flow of gases to equalize pressure • Consists of two phases • Inspiration – air flows into the lungs • Expiration – gases exit the lungs
Pressure Relationships in the Thoracic Cavity • Respiratory pressure is always described relative to atmospheric pressure • Atmospheric pressure (Patm) • Pressure exerted by the air surrounding the body • Negative respiratory pressure is less than Patm • Positive respiratory pressure is greater than Patm • Intrapleural pressure (Pip) – pressure within the pleural cavity • always less than intrapulmonary pressure and atmospheric pressure • Intrapulmonary pressure (Ppul) – pressure within the alveoli • eventually equalizes itself with atmospheric pressure
Intrapleural Pressure and Pressure Relationships • Negative Pip is caused by opposing forces • Two inward forces promote lung collapse • Elastic recoil of lungs decreases lung size • Surface tension of alveolar fluid reduces alveolar size • One outward force tends to enlarge the lungs • Elasticity of the chest wall pulls the thorax outward • If Pip = Ppul the lungs collapse • (Ppul – Pip) = transpulmonary pressure • Keeps the airways open
Intrapleural pressure • As a result of the relationship between the lungs and the pleurae (lungs pull the visceral pleura in), the intrapleural pressure is below atmospheric pressure – average of -4 mmHg • This pressure (or the fluid bond between the pleurae) prevents the collapsing of the lungs due to there elasticity
Pulmonary ventilation – inspiration and expiration • Pulmonary ventilation depends on volume changes in the thoracic cavity • Volume changes lead to pressure changes • Pressure changes lead to flow of gases • Boyle’s Law- The volume of a fixed amount of gas is inversely proportional to the total amount of pressure applied. • If the pressure doubles, the volume shrinks to half. • In the lungs – if lungs volume increase the pressure decreases (intrapulmonary pressure)
Modes of breathing • Quiet breathing – eupnea • Inhalation is active and exhalation is passive (relaxation of muscles) • Forced breathing – hyperpnea • Both inhalation and exhalation involve muscle contraction – both active • Inhalation involve muscles like the pec. minor, sternocleidomastoid and more • Exhalation involves the internal intercostals and abdominal muscles among others
Physical Factors Influencing Ventilation • 3 factors influence pulmonary ventilation • Airway Resistance • Alveolar Surface Tension • Lung Compliance
Airway Resistance • As airway resistance rises, breathing movements become more difficult • Resistance is usually insignificant because of • Large airway diameters in the first part of the conducting zone • Progressive branching of airways as they get smaller, increasing the total cross-sectional area • Severely constricted or obstructed bronchioles: • Can prevent life-sustaining ventilation • Can occur during acute asthma attacks which stops ventilation • Epinephrine release via the sympathetic nervous system dilates bronchioles and reduces air resistance
Alveolar Surface Tension • Surface tension – the attraction of liquid molecules to one another at a liquid-gas interface • The liquid coating the alveolar surface is always acting to reduce the alveoli to the smallest possible size • Surfactant, a detergent-like complex, reduces surface tension and helps keep the alveoli from collapsing • Normally, surfactant synthesis starts at about the 25th week of fetal development and production reaches optimal levels at 34th week • Premature babies with insufficient surfactant can be treat with aerosol administration with artificial surfactant until lungs mature
Lung Compliance • Compliance is the indication of the lungs expandability • The ease with which lungs can be expanded • Factors that diminish lung compliance • Scar tissue or fibrosis that reduces the natural elasticity of the lungs • Blockage of the smaller respiratory passages with mucus or fluid • Reduced production of surfactant • The mobility of the thoracic cage – changes cause to the articulations of the ribs or to the muscles involved.
Respiratory Volumes • Used to assess a person’s respiratory status • Tidal volume (TV) • Inspiratory reserve volume (IRV) • Expiratory reserve volume (ERV) • Residual volume (RV)
Adult female average value Adult male average value Measurement Description Amount of air inhaled or exhaled with each breath under resting conditions Tidal volume (TV) 500 ml 500 ml Amount of air that can be forcefully inhaled after a nor- mal tidal volume inhalation Inspiratory reserve volume (IRV) 3100 ml 1900 ml Respiratory volumes Amount of air that can be forcefully exhaled after a nor- mal tidal volume exhalation Expiratory reserve volume (ERV) 1200 ml 700 ml Amount of air remaining in the lungs after a forced exhalation Residual volume (RV) 1200 ml 1100 ml Figure 22.16b
Respiratory Capacities • Inspiratory capacity (IC) equals TV plus IRV • Maximum amount of air (about 3.5 liters) a person can breath in • Functional residual capacity (FRC) equals the ERV plus RV • Amount of air remains in the lungs at the end of normal expiration • Vital capacity (VC) equals IRV+ERV+TV • Maximum amount of air a person can expel from the lungs after filling with inspiratory capacity • Total lung capacity (TLC) equals VC+RV • Maximum volume to which the lungs can be expanded
Maximum amount of air contained in lungs after a maximum inspiratory effort: TLC = TV + IRV + ERV + RV Total lung capacity (TLC) 6000 ml 4200 ml Maximum amount of air that can be expired after a maxi- mum inspiratory effort: VC = TV + IRV + ERV Vital capacity (VC) 4800 ml 3100 ml Respiratory capacities Maximum amount of air that can be inspired after a normal expiration: IC = TV + IRV Inspiratory capacity (IC) 3600 ml 2400 ml Volume of air remaining in the lungs after a normal tidal volume expiration: FRC = ERV + RV Functional residual capacity (FRC) 2400 ml 1800 ml (b) Summary of respiratory volumes and capacities for males and females Figure 22.16b
Dead Space • Some of the inspired air does not contribute to the gas exchange in the alveoli • Anatomical dead space – volume of the conducting respiratory passages (150 ml) • Alveolar dead space – alveoli that cease to act in gas exchange due to collapse or obstruction • Total dead space – sum of alveolar and anatomical dead spaces • On expiration, the air in the anatomical dead space is expired first
Pulmonary Function Tests • Spirometer – an instrument used to evaluate respiratory function • Spirometry can distinguish between: • Obstructive pulmonary disease – increased airway resistance by narrowing or blocking airways (ex. Asthma) • Restrictive disorders – reduction of pulmonary compliance thus limiting inflation of lungs. • Caused by any disease that produces pulmonary fibrosis
Nonrespiratory Air Movements • Most result from reflex action • Examples include: coughing, sneezing, crying, laughing, hiccupping, and yawning
Respiratory physiology is a series of integrated processes • External respiration • Exchange of gases between blood and the external environment • Internal respiration • Exchange of gases between blood and interstitial fluid • Transport of oxygen and carbon dioxide • To understand the above processes, first consider • Physical properties of gases • Composition of alveolar gas
Basic properties of gases • Dalton’s Law of Partial Pressures • Total pressure exerted by a mixture of gases is the sum of the pressures exerted independently by each gas in the mixture (as if no other gases were present) • The separate contribution of each gas in a mixture is called partial pressure (symbolized with P) • The partial pressure of each gas is directly proportional to its percentage in the mixture
Composition of air in alveoli • The composition of air we breath is not the composition in the alveoli: • The air is humidified by the contact with the mucus membrane – so PH2O is >10 times higher than the inhaled air • Freshly inspired air is mixed with residual air left from previous breathing cycle • That causes the oxygen to be diluted and CO2 to be higher • Alveolar gas exchanges O2 and CO2 with blood • As a result, PO2 of alveolar air is about 65% of that of the inhaled air and PCO2 is >130 higher
Alveolar gas exchange Diffusion between liquid and gases (Henry’s law) • When a mixture of gases is in contact with a liquid, each gas will dissolve in the liquid in proportion to its partial pressure • The greater the concentration of a particular gas, the more and the faster that it will go into a solution • The amount of gas that will dissolve in a liquid also depends upon its solubility: • Carbon dioxide is the most soluble • Oxygen is 1/20th as soluble as carbon dioxide • Nitrogen is practically insoluble in plasma
External Respiration: Pulmonary Gas Exchange • Factors influencing the movement of oxygen and carbon dioxide across the respiratory membrane (what is the respiratory membrane?) • Partial pressure gradients and gas solubility • Matching of alveolar ventilation and pulmonary blood perfusion • Structural characteristics of the respiratory membrane
Partial Pressure Gradients and Gas Solubility • The partial pressure oxygen (PO2) of venous blood is 40 mm Hg; the partial pressure in the alveoli is 104 mm Hg • This steep gradient allows oxygen partial pressures to rapidly reach equilibrium (in 0.25 seconds) • this is one third of the time a RBC is in the pulmonary capillary (0.75 seconds) • Although carbon dioxide has a lower partial pressure gradient (45 mm Hg in the blood and 40 mm Hg in the alveoli; a gradient of 5 mm Hg): • It diffuses in equal amounts with oxygen because it is 20 times more soluble in plasma than oxygen
Surface Area and Thickness of the Respiratory Membrane • The amount of gas that moves across a tissue is • proportional to the area of the sheet • inversely proportional to its thickness • Respiratory membranes: • Are only 0.5 to 1 m thick, allowing for efficient gas exchange • Have a total surface area of about 60 m2 (40 times that of one’s skin)
Internal Respiration • The factors promoting gas exchange between systemic capillaries and tissue cells are the same as those acting in the lungs • The partial pressures and diffusion gradients are reversed • PO2 in tissue is always lower than in systemic arterial blood • PO2 of venous blood draining tissues is 40 mm Hg and PCO2 is 45 mm Hg
Oxygen Transport: Role of Hemoglobin • Molecular oxygen is carried in the blood: • Bound to hemoglobin (Hb) within red blood cells • Dissolved in plasma (O2 has low solubility in water and only 1.5% is dissolved in plasma) • Each Hb molecule binds four oxygen atoms in a rapid and reversible process • The hemoglobin-oxygen combination is called oxyhemoglobin (HbO2) • Hemoglobin that has released oxygen is called reduced hemoglobin/deoxyhemoglobin (HHb) • Saturated hemoglobin – when all four hemes of the molecule are bound to oxygen • Partially saturated hemoglobin – when one to three hemes are bound to oxygen
The Oxygen-Hemoglobin Saturation Curve • PO2 of 40 mm Hg – (average in the tissues) Hb is 75% saturated • only 25% of the O2 is unload from Hb in resting conditions • PO2 of 60-70 mm Hg – Hb is 90% saturated • PO2 of 20 mm Hg – Hb is only 30% saturated • Ex. – active muscle; relatively high percentage of O2 released with small decrease in Po2
Factors That Increase Release of Oxygen by Hemoglobin • As cells metabolize glucose, carbon dioxide is released into the blood causing: • Increases in PCO2 and H+ concentration in capillary blood • Declining pH (acidosis), which weakens the hemoglobin-oxygen bond (Bohr effect) • Metabolizing cells have heat as a byproduct and the rise in temperature increases BPG synthesis • All these factors ensure oxygen unloading in the vicinity of working tissue cells
Carbon Dioxide Transport • Carbon dioxide is transported in the blood in three forms • Dissolved in plasma – 7 to 10% • Chemically bound to hemoglobin – 20% is carried in RBCs as carbaminohemoglobin • Bicarbonate ion in plasma – 70% is transported as bicarbonate (HCO3–)
Carbon Dioxide Transport • In areas with high PCO2, carbon dioxide leaves the cell, diffuses through the interstitial fluid and enters a capillary. • Most of it enters an erythrocyte that contains an enzyme, carbonic anhydrase which catalyses the following reaction: • CO2 + H20 -----> H2CO3 -----> H+ + HCO3-- . • The bicarbonate ion leaves the red blood cell (against concentration gradient) and travels to the lungs in the plasma of the blood. • In exchange, Cl- moves from plasma into RBCs to maintain the electrical balance between plasma and RBC (chloride shift) • It often combines with Na+ present in the plasma to form sodium bicarbonate which plays a role in maintaining the homeostasis of blood pH.