Download
1 / 34
340 likes | 502 Views
Know Your Clients: Challenges in Integrating Family Planning into Ethiopian VCT Clinics. Wednesday Noon Seminar Series Department of Population, Family and Reproductive Health September 23, 2009. Duff Gillespie, PhD Heather Bradley, PhD Candidate

E N D
Know Your Clients: Challenges in Integrating Family Planning into Ethiopian VCT Clinics Wednesday Noon Seminar Series Department of Population, Family and Reproductive Health September 23, 2009 Duff Gillespie, PhD Heather Bradley, PhD Candidate Johns Hopkins Bloomberg School of Public Health The Bill and Melinda Gates Institute for Population and Reproductive Health dgillesp@jhsph.edu
Rationale for HIV and FP service integration Common mode of transmission for unintended pregnancy and HIV. May increase programmatic effectiveness and efficiency. More than 60 percent of HIV-infected adults in sub-Saharan Africa are childbearing-aged females. Offering family planning services within the context of VCT may reduce unintended pregnancies among HIV-positive persons.
HIV and FP service integration: an evidence-based policy? • Most donors and governments have policies encouraging reproductive health and HIV service integration. • Based on the assumption that both service types target individuals with sexual risk behavior. • Previous operations research suggests unmet contraceptive need among VCT clients. • No study to date has shown integration increases contraceptive uptake among VCT clients.
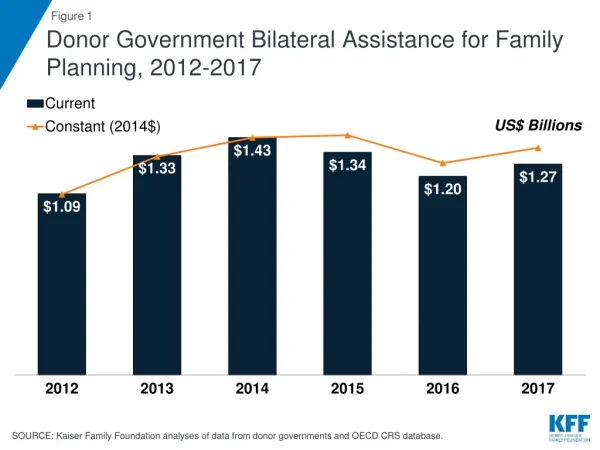
PEPFAR funding in Ethiopia $851 million over past 5 years PEPFAR country fact sheet, FY2008
VCT in Ethiopia HIV prevalence is 2.1% (over 1 million persons infected), much higher in urban areas (7.7%). VCT facilities increased from 658 in 2004 to 1,469 in 2008. Number of HIV tests increased from 448,000 in 2004 to 4.6 million in 2008. Millennium AIDS Campaign launched in 2006 to increase testing among the general population. Broad, non-specific outreach messages “know your status, plan for your future”
HIV and FP service integration in Ethiopia Government of Ethiopia’s current HIV policy endorses integration of reproductive health and VCT, PMTCT and ARV services. Ethiopian task force created to promote HIV and FP integration in response to WHO-sponsored International Best Practices meeting. Task force included Ministry of Health and NGO partners, led by Pathfinder International-Ethiopia. Aimed to initiate integrated services in 20% of VCT and PMTCT service sites in four focus regions.
VICS Study Aims • Estimate the need and demand for family planning among VCT clients in eight Oromia Region public sector facilities. • Assess clients’ contraceptive uptake in VCT sessions. • Determine what kinds of clients received contraceptive counseling and/or methods.
Study Design Cross-sectional study, pre- and post-intervention (before and after family planning services are made available in VCT counseling sessions). VCT clients were interviewed in 8 public sector facilities. Clients interviewed twice: 1) after pre-test HIV counseling, 2) after post-test HIV counseling. Total sample size=8,046 clients 4,019 pre-intervention, 4,027 post-intervention
FP/HIV integration intervention Training and authorizing public sector VCT counselors to offer pills, condoms and injectables to clients during VCT sessions. Ensuring continuous contraceptive supplies to facilities, including pills, condoms, injectables, Norplant and IUDs. Developing specialized family planning counseling messages for VCT clients, which apart from married couples, target youth, singles and engaged couples.
VICS Two Main Outcome Variables • The client received contraceptive counseling during VCT • The client obtained a contraceptive method during VCT
Statistical methods Examined client characteristics Demographic variables Contraceptive use Unmet contraceptive need Regressed study outcomes on client, provider and facility-level variables using multi-level logistic models Post-intervention sample Linked clients to providers and facilities Excluded clients from one facility due to inadequate implementation Random intercepts for facilities and providers
VCT client characteristics after introduction of family planning services
VCT clients’ level of sexual activity after introduction of family planning services: male and female clients (%)
VCT clients’ contraceptive use before and after introduction of family planning services: male and female clients who have ever had sex (%)
Unmet need for contraception among clients interviewed post-intervention: married women and those reporting sex in the past 30 days Total unmet need=17%
Counseling topics discussed before and after introduction of family planning services: HIV-negative VCT clients *significant at p<0.05 level
Counseling topics discussed before and after introduction of family planning services: HIV-positive VCT clients *significant at p<0.05 level
Percentage of clients receiving family planning counseling in VCT before and after introduction of family planning services Men Women * * N=1,187 N=1,643 N=1,192 N=1,731 *significant at p<0.05 level
Percentage of clients receiving a family planning method in VCT before and after introduction of family planning services: male and female clients
Percentage of clients receiving family planning counseling in VCT by couples’ counseling AOR=3.4 (p<0.01) AOR=1.0 Men Women N=1,460 N=271 N=1,390 N=253
Percentage of clients receiving a family planning method in VCT by level of sexual activity Men Women AOR 4.0 (p<0.01) AOR 11.8 (p<0.01) AOR 5.1 (p<0.01) AOR 1.8 (p<0.08) AOR1.0 AOR 1.0 N=482 N=793 N=368 N=676 N=557 N=498
Percentage of clients receiving a family planning method in VCT by primary reason for HIV testing Men Women N=767 N=551 N=325 N=645 N=681 N=405
Percentage of clients receiving a family planning method in VCT by whether client received contraceptive counseling Men Women AOR 3.9 (p<0.01) AOR 6.0 (p<0.01) AOR 1.0 AOR 1.0 N=1,175 N=468 N=1,028 N=703
Percentage of clients receiving a family planning method in VCT by counselor assessment of FP supplies Women Men AOR 2.2 (p<0.01) AOR 4.3 (p<0.01) AOR 1.0 AOR 1.0 N=794 N=849 N=800 N=931
Why do clients who are not sexually active test for HIV? • Of VCT clients* who have never had sex: • 99% know that HIV is a sexually transmitted infection. • But… • 95% believe “sometimes people are infected with HIV for no apparent reason.” • 79% believe people who abstain from sex are not protected from HIV. • 92% say HIV testing helps them to worry less about HIV. • *Clients testing for pre-marital or visa purposes excluded.
Clients believe HIV can be transmitted in many ways, many outside their control. • “It does not come to you by thinking about it. It is just a happening, not a problem…HIV doesn’t come because you wanted it, for instance it comes through accidents and by sharp materials. It is not only through sex. That makes it a happening. The sharp material cuts them by accident, it is not because they want it, it just happens.” • - Female VCT client, single/non-sexually active, age 15
Clients fear HIV-infection through “unknown means.” • “Although I protect myself from HIV and live a careful life, it may catch me suddenly through unknown means…You cannot be sure fully outside of the test. For this reason it will help me in my future life that is why I came to take the test.” • - Male VCT client, single/non-sexually active, age 18
Clients fear intentional infection by HIV-positive persons. • “In our locality, we hear that some ladies put their menstruation in tella [a home-brewed alcoholic beverage] and give to people to transmit the disease…They think, because I am a carrier [of HIV], others should be also infected. I think this is the culture some Ethiopians have.” • - Female VCT client, married, age 19
Testing for HIV helps clients to manage fear. • “As I have told you before, HIV contamination may occur unexpectedly. But when you prove yourself free of the contamination again then you will develop your self-confidence again.” • –Female VCT client, single/non-sexually active, age 19
Testing for HIV helps clients to manage fear - 2 • “It [HIV testing] makes me lead my future life joyfully and according to plan…You feel happy for a while if you know you are free.” • - Female VCT client, single/non-sexually active, age 19
VICS – Summary of Findings • Programmatically, family planning was successfully integrated into VCT services. • Family planning acceptance increased, but… • Unmet contraceptive need was low (17%). • It is likely that contraceptive uptake would have been higher among a more sexually active population. • An outreach campaign focusing on higher risk groups would attract more persons in need of both VCT and family planning services.
Acknowledgements Research partners Pathfinder International-Ethiopia Miz-Hasab Research Center Funding support from The David and Lucile Packard Foundation The William and Flora Hewlett Foundation The Bill and Melinda Gates Institute for Population and Reproductive Health Appreciation to Chandrakant Ruparelia, Jhpiego, Baltimore, MD Yung-Ting Bonnenfant, JHSPH, Baltimore, MD