Download
1 / 42
420 likes | 491 Views
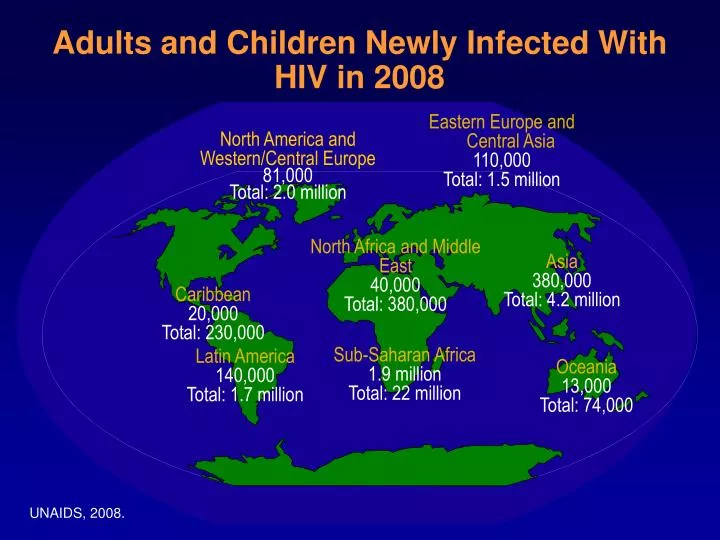
Adults and Children Newly Infected With HIV in 2008. Eastern Europe and Central Asia 110,000 Total: 1.5 million. North America and Western/Central Europe 81,000 Total: 2.0 million. North Africa and Middle East 40,000 Total: 380,000. Asia 380,000 Total: 4.2 million.

E N D
Adults and Children Newly Infected With HIV in 2008 Eastern Europe and Central Asia 110,000 Total: 1.5 million North America and Western/Central Europe 81,000 Total: 2.0 million North Africa and Middle East 40,000 Total: 380,000 Asia 380,000 Total: 4.2 million Caribbean 20,000 Total: 230,000 Sub-Saharan Africa 1.9 million Total: 22 million Latin America 140,000 Total: 1.7 million Oceania 13,000 Total: 74,000 UNAIDS, 2008. http://www.unaids.org.
Human Immunodeficiency Viruses • HIV-2 • HIV-2 is less virulent and less transmissible • HIV-2 is closely related to SIVsm, found in Sooty Mangebey monkeys • HIV-2 is epidemic in Western Africa, India • HIV-1 • HIV-1 is more virulent and more transmissible • HIV-1 is closely related to SIVcpz, found in Chimpanzees • HIV-1 is pandemic • HIV-1 strains are divided into three groups (M - main, N, O - outlier) • HIV-1 group M is divided into several subtypes (Clades A through J)
Global HIV Estimates • Cumulative HIV-1 infections = 80 million • Persons living with HIV-1 • Adults 40 million • Children 2.7 million • New HIV-1 infections yearly • Adults 5 million • Children 0.9 million • AIDS Orphans • 14 million • 20 million by 2010
Global Burden of HIV-1 Infection in Women • Half of all new infections occur in women • Half of the 40 million individuals living with HIV are women • Sub-Saharan Africa: 60% (75% ages 15-24) • Caribbean: 50% • Latin America: 35% • South/SE Asia: 30% Quinn and Overbaugh, Science 308: 1582, 2005
Where do we find HIV? • Blood • Seminal fluid • Vaginal fluid • Breast milk • Saliva • Tears • Urine/feces
How is it transmitted (cont) • Use of unclean needles for drug use including steroids, piercing • From HIV+ mother to unborn child • Contaminated blood products • Needlesticks
Who is at risk for HIV? • Men who have unprotected sex with men • Men who have unprotected sex with men and women • Men/women who use unclean needles • Women who have unprotected sex with women who are menstruating • Women who have unprotected sex with men
What age groups are vulnerable? • Women have represented approximately 50% of cases of HIV in Africa all along • In the US, women were only 5% in the 1980’s now approaching 50% • Fastest growing numbers of new cases in ages 13-24 and over 50 • Men who have sex with men have begun to represent an upward spiral of new cases
Cellular CD4 receptor CD4 ( T Helper) Cell Human DNA chromosome
Reverse transcriptase Integrase Protease gp120 gp41 HIV HIV RNA chromosome CD4 ( T Helper) Cell Cellular CD4 receptor Human DNA chromosome
4. Fusion of cell and virus 2. Gp120-CD4 interaction 3. Conformational change in gp120, exposing hydrophobic fusion protein (harpoon) of gp41 1. HIV approaches CD4 cell
CD4 ( T Helper) Cell Reverse transcriptase Cellular CD4 receptor Integrase Protease gp120 gp41 HIV RNA chromosome Human DNA chromosome
CD4 ( T Helper) Cell Reverse transcriptase Cellular CD4 receptor Integrase Protease gp120 gp41 RNA nucleotides HIV RNA chromosome Human DNA chromosome
CD4 ( T Helper) Cell Reverse transcriptase Cellular CD4 receptor Integrase Protease gp120 gp41 RNA nucleotides DNA nucleotides HIV RNA chromosome Human DNA chromosome
CD4 ( T Helper) Cell Reverse transcriptase Cellular CD4 receptor Integrase Protease gp120 gp41 HIV RNA chromosome HIV DNA provirus Human DNA chromosome
CD4 ( T Helper) Cell Reverse transcriptase Cellular CD4 receptor Integrase Protease gp120 gp41 Reverse Transcriptase Inhibitors:Nucleoside and Non-Nucleosides HIV RNA chromosome Human DNA chromosome
CD4 ( T Helper) Cell Reverse transcriptase Cellular CD4 receptor Integrase Protease gp120 gp41 HIV RNA chromosome HIV DNA provirus Human DNA chromosome
CD4 ( T Helper) Cell Reverse transcriptase Cellular CD4 receptor Integrase Protease gp120 gp41 Cellular Activation HIV RNA chromosome HIV DNA provirus Human DNA chromosome
HIV Protease gp120 gp41 Functional proteins Protease Inhibitors Non-functionalgp160 precursor
HIV CD4 ( T Helper) Cell Reverse transcriptase Cellular CD4 receptor Integrase Protease gp120 gp41 HIV RNA chromosome HIV DNA provirus Human DNA chromosome
CD4 Cell Count and Viral Load • CD4 cell count • The number of T helper cells, or CD4 cells, in your blood. The count is measured as the number of cells per cubic millimeter (cells/mm3). Higher CD4 cells counts are a sign of a healthier immune system. Levels below 1000 indicate that the immune system is impaired. Blood tests measuring CD4 cells can help to determine if HAART is working. • Viral Load • The number of viruses circulating in your blood. Measured as counts per milliliter (c/mL or counts/mL). 1 milliliter = a cubic centimeter. Counts of 50 and below are termed “undetectable”. Blood Test: Viral Load also used to indicate whether HAART is Working/resistance is developing
90,000 80,000 70,000 60,000 50,000 40,000 30,000 20,000 10,000 0 Number of AIDS cases and number of deaths from AIDS in the USA 1981-2001 400,000 300,000 Number of deathsfrom AIDS/year Number of new AIDS cases/year Total number of AIDS cases 200,000 100,000 0 81 85 90 95 00 01 Year 10th CROI, Boston 2003, #4; Incidence and deaths data from the CDC
1996 2004 1987 When to Start Therapy? CD4 lymphocytes HIV RNA load Treatmentinitiation in: 6–24 weeks 0.5–15 (?) years 2–3 years Infection with HIV Clinical AIDS Original slide courtesy of Dr Sven A. Danner.
Updated IAS-USA Guidelines: When to Start *Non-AIDS risk factors include HIV-associated nephropathy, hepatitis C, hepatitis B Hammer SM, et al. JAMA. 2008;300:555-570.
High A partially effective regimen Resistance A highly effective regimen Low Low High Adherence Start on the most potent drug to keep the virus down • 100% adherence to a partially effective regimen will still result in virologic failure due to resistance • With a highly effective regimen, resistance is highest when adherence is intermediate • To avoid resistance: • Pr0viders should use a potent medication that will achieve maximum suppression of the virus and that the patient can strictly stick to • The patient should adhere to the regimen Adapted from Bangsberg DR, et al. XI International HIV Drug Resistance Workshop. Seville, 2002. #160
News on metabolic side effects News in brief • Triglycerides • In 23 patients (of ~1300 patients) who had received HAART from 1997-2003 and who had developed high trigs: • Severe high trigs were more likely in patients receiving high dose ritonavir (more than 300 mg per day) • High trigs above 1000 mg/dL is associated with pancreatitis • There were no cases of pancreatitis associated with high trigs in this study • Abnormal fat distribution • A diet rich in polyunsaturated fats may help to reduce cell death which has been correlated with abnormal fat distribution as a side effect of HIV meds – the implications are unknown as this study was done in the laboratory and not in patients • Avascular necrosis • Smoking is a risk factor for avascular necrosis in HIV-infected patients • Cardiovascular • Smoking was the most frequent indicator of CV risk for patients on HAART. Other considerations included : lower CD4 nadir, male gender, protease inhibitor use. 43rd ICAAC, Chicago 2003, #H-1947, #H-1948, #H-1956, #H-1958
Risk Factors: Lipodystrophy • Age > 40 years • Hx of AIDS > 3 years • CD4+ nadir < 100 or CD4+% nadir < 15% • Body mass index (BMI) loss of ≥ 1 kg/m2 • BMI change of ≥ 2 kg/m2 • White race • Duration of Rx with indinavir or stavudine associated with increased risk of lipodystrophy Lichtenstein KA, et al. J Acquir Immune Defic Syndr. 2003;32:48-56.
Lipoatrophy Risk: Dual NRTI + PI vs Dual NRTI Risk of lipoatrophy with 2 NRTI + PI greater than with 2 NRTI alone 1.0 0.8 2 NRTIs 0.6 probability of remaining free of subcutaneous lipoatrophy 2 NRTIs + PI 0.4 0.2 0.0 0 200 400 600 800 1000 time (days) from start of dual therapyto lipoatrophy Mallal SA. AIDS 2000;14:1309
+30 +15 0 -15 -30 Median % change from BL 0 24 48 72 96 120 144 Week central abdominal fat limb fat lean mass Evolution of body fat over time,following initiation of ART • Australian lipodystrophy cohort starting HAART • measurements by DEXA: • initial increase in central and peripheral fat • limb fat declines from baseline after ~1yr • central abdominal fat remains increased from baseline Mallon PWG, et al. AIDS 2002;
GS 903 Study:Patients (%) with Lipodystrophy+ TDF+3TC+EFV d4T+3TC+EFV * * % Patients with Selected Toxicities * * Week 48 Week 96 Week 144 +Investigator-defined * p value < 0.001
Metabolic Syndrome • Many different definitions of the metabolic syndrome • Prevalence and association with HIV infection may be dependent on choice of definition • WIHS: found higher prevalence of metabolic syndrome in HIV-infected women, but factors significantly associated with metabolic syndrome were traditional risk factors (age, race, higher BMI, smoking), not HIV related[1] • MACS: HIV-infected men who are treated have larger waists as they age; reversal of previous decrease in waist size with NRTI treatment[2] 1. Sobieszczyk ME, et al. IAC 2006. Abstract WEPE0147. 2. Brown T, et al. IAC 2006. Abstract WEPE0136.
Australian Prevalence Study; buffalo hump was found in 2% of HIV+ Buffalo hump (BH) and associated metabolic abnormalities • Buffalo hump is commonly found in overweight people and is associated with metabolic changes seen in overweight individuals - insulin resistance and larger body mass index • Presence of BH is not associated with high blood lipids, e.g. triglycerides, cholesterol 1. Miller M, HIV Med 2003; 4:293-301; Mallon PWG, et al.2nd IAS, Paris 2003, #715
Treatment Plan- Individualized • Pill burden • Number of doses per day • Lifestyle issues • Side effects • Effectiveness (potency and durability) • Preserving future options(sequencing) • Provide adherence support
Advances in current treatment and care: Summary • Once-daily combinations • No required water or food • Many can be stored in cool areas but no need for refrigeration • Side effects less gastrointestinal but more metabolic
How Much Adherence is Needed? (number of pills taken / number of pills prescribed) Ann Intern Med 2000;133:21
What is treatment failure? • When antiretroviral medications stop controlling HIV,viral load goes up and CD4 counts go down • Immune damage continues • Risk of an opportunistic infection increases • Drug resistance is a major cause of treatment failure.
Nurses and HIV • Leaders • Educators • Counselors /Testers • Treatment managers • Adherence coaches • Symptom managers • Prevention counselors