Download
1 / 47
470 likes | 477 Views
Intimate Partner Violence: Urgent Implications for Women's Health. Nancy Glass, PhD, MPH, RN Co-Director, Center for Health Disparities Research Oregon Health & Science University www.ohsu.edu/healthdisparities/. Objectives. Define intimate partner violence (IPV).

E N D
Intimate Partner Violence: Urgent Implications for Women's Health Nancy Glass, PhD, MPH, RN Co-Director, Center for Health Disparities Research Oregon Health & Science Universitywww.ohsu.edu/healthdisparities/
Objectives • Define intimate partner violence (IPV). • Describe the overlap of forms of IPV. • Describe the prevalence of this public health problem. • Describe physical, psychosocial and pregnancy related effects of IPV.
Objectives • Discuss use of assessment tools in clinical practice. • Identify local and national resources for women in abusive relationships.
Definition: Intimate Partner Violence • Centers for Disease Control and Prevention (CDC) • Physical and/or sexual violence (use of physical force) or threat of such violence; or psychological/ emotional abuse and/or coercive tactics when there has been prior physical and/or sexual violence; between persons who are spouses or non marital partners (dating, boyfriend-girfriend, same-sex) or former spouses or non marital partners (Saltzman et.al. ‘99)
Definition: Intimate Partner Violence • Conceptualized as a risk factor for many health problems rather than a disease or syndrome or diagnosis.
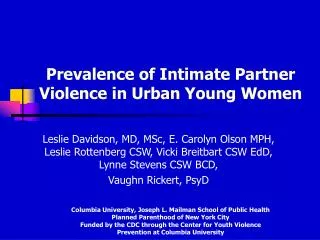
Intimate Partner Violence Population-based telephone survey (N=8000 women) (Tjaden & Thoennes, 1998) 25% of women reported lifetime physical and/or sexual assault by an intimate or ex-intimate partner Estimated 4.8 million women report physical/sexual violence from an intimate in the past year. 40% of assaults result in injuries 20% seek health care services related to the assault 10% of Oregon women report physical/sexual violence from an intimate in the past year (Oregon DHHS).
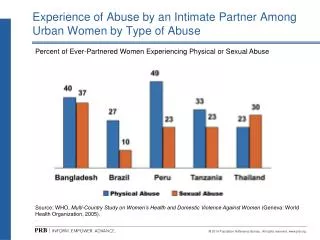
Overlap between physical, sexual and emotional abuse (N = 889) (Campbell et. al. ’02) Sexual (N = 243) 32 (3.6) 31 (3.5) 14 (1.6) 166 (18.7) 177 (19.9) 166 (18.7) 303 (34.0) Emotional (N = 677) Physical (N = 649)
General Health Outcomes • Serious health outcomes, last long after the violence has ended. • Survivors of IPV report poorer overall health status, poorer quality of life, and functional status as compared to women who report never experiencing IPV (Glass 2001, Sullivan et al., 1999; Plichta, 1996).
Health Effects - 5 Major Studies(controlled, pop based or large HMO – Campbell et. al. ’02; Coker et.al.’00; Leserman et.al.’98; McCauley et.al.’95; Plichta ‘96)
Health Effects - 5 Major Studies(controlled, pop based or large HMO – Campbell et. al. 02; Coker et.al.’00; Leserman et.al.’98; McCauley et.al.’95; Plichta ‘96)
Mental Health Outcomes • Depression and Post Traumatic Stress Disorder (PTSD) most commonly reported mental health outcome of IPV (Campbell, 2001; Glass, 2001; Campbell et al., 1997; Campbell et al., 1995) • 59.2% of injured women from a Level 1 Trauma Center reported symptoms of PTSD (up to 5 years after the injury) (Glass, 2001) • Relationship between IPV and suicidiality (McCauley et al., 1995)
Mental Health Outcomes • Substance Use (ETOH, illegal drugs, prescription drugs). (Sharps et al., 2001) • Women with depression and/or PTSD may use substances to calm, cope with all three PTSD specific symptoms clusters (intrusion, avoidance, and hyperarousal) • Dangerous reciprocal relationship between violence re-victimization and substance use (Dansky et al., 1997)
Health Care Utilization • Examined relationship of IPV and health care utilization in population and clinical studies has revealed; poorer overall physical and mental health, higher incidence of injuries, increase consumption of health care resources (hospitalization, health visits, prescriptions) (McCauley et al., 1995; Campbell et al., 2001). • Although there is an increased use of health care by abused women, only 20% are correctly identified (Campbell et al., 2002)
Prevalence: Pregnancy-Related Violence • IPV during pregnancy range from 0.9% to 20.1% (Gazmararian et al., 1996) • The majority of studies, the prevalence estimate has ranged from 4%-8% • Wide range of prevalence estimates likely the results of a variety of measures, populations sampled and methodology
Oregon Prevalence: Pregnancy Related Violence • Findings are based on the results of the 2000 Oregon DHS Pregnancy Risk Assessment Monitoring System (PRAMS) • Ongoing survey of women who have recently given birth. • 2,100 new mothers participated in the representative sample
Oregon Prevalence: Pregnancy-Related Violence • “During your recent pregnancy did your husband or partner push, hit, slap, kick, choke or physically hurt you in any other way" • 2.6% of respondents answered YES • Additionally, 0.8% of respondents, reported that someone else had physically hurt them while they were pregnant (ex-partner, ex-boyfriend) • 1,472 new mothers reported being physically hurt while pregnant in 2000
Oregon Prevalence: Pregnancy Related Violence • In addition to violence during the pregnancy: • 3.8% of respondents reported being physically hurt by their husband or partner in the 12 months before they became pregnant • Another, 1.6% of respondents, reporting being physically hurt by someone else in the 12 months before they became pregnant • 2,339 new mothers reporting being physically hurt in the year prior to the pregnancy
Pregnancy and Violence • Public health perspective, an important question is risk patterns to develop prevention programs to reduce IPV during pregnancy • “Are pregnant women at a greater risk of physical/sexual violence by their male partners or ex-partners compared to women who are not pregnant?” • Studies using national probability samples (e.g. National Family Violence Survey, 1985; 1992 National Alcohol and Family Violence Survey; National Survey of Families and Households, 1988) have indicated that pregnant women were no more likely to be victims of IPV than women who were not pregnant • In one survey, National Survey of Families and Households, 1988, persistent violence was more likely to occur among couples in which the male partner perceived that the pregnancy of his female partner occurred sooner than intended
Risk Factors for Pregnancy-Related Violence • Cumulative effect of multiple contextual and relationship factors and stressors, can impact parental perception of newborns, family environment, attitudes toward parenting, and levels of relationship discord (Fisher et al., 1998)
Consequences of Pregnancy-Related Violence • Consequences for both the unborn child and pregnant mother: • Late entry into prenatal care • Low birth weight babies • Premature labor • Unhealthy maternal behaviors • Fetal trauma • Health issues for the mother
Consequences of Pregnancy-Related Violence • Late entry into prenatal care • Healthy People 2010, 90% of pregnant women will begin prenatal care in first trimester • Abused women are twice as likely to delay prenatal care until the 3rd trimester compared to women who were not abused (Goodwin et al., 2000) • Late entry to prenatal care is a risk factor for pregnancy complications including low birth weight babies and premature labor
Consequences of Pregnancy-Related Violence • Low birth weight and Premature Labor • Studies have been inconsistent in findings related to the association between IPV, premature labor and low birth weight infants (Curry & Harvey, 1998; Cokkinides et al., 1999). • In addition to IPV, low birth weight and premature labor may be associated with late entry into prenatal care, as well as unhealthy behaviors by the mother (e.g. smoking, poor nutrition)
Consequences of Pregnancy-Related Violence • Fetal Trauma (e.g miscarriage, spontaneous abortion) • Experiencing IPV puts the unborn baby at risk • Increased risk of miscarriage (Jacoby et al., 1999) • Association between current IPV and at least one spontaneous abortion in the woman’s obstetric history (Jacoby et al., 1999) • Increased risk of placental abruptions (Connolly et al., 1997)
Consequences of Pregnancy-Related Violence • Unhealthy Maternal Behaviors • IPV indirect contribution to negative consequences for both unborn child and mother by increasing the risk for unhealthy maternal behaviors • Abused women are more likely to smoke during pregnancy than women who are not abused (Cokkinides & Coker, 1998) • Prenatal patients (n=2000), victims of IPV were more likely to smoke, drink and use drugs than women who were not abused (Martin et al., 1996) • IPV victims were more likely to be in the most severe substance abuse category during pregnancy than nonabused women (Martin et al., 1996)
Consequences of Pregnancy-Related Violence • Health Issues for Mothers • Unhealthy diet, severe postpartum depression, lower self-esteem, breastfeeding difficulties, anemia and poor weight gain have all been associated with IPV and pregnancy (Bohn & Holz, 1996)
Femicide • Femicide, murder of women • 7th leading cause of premature death for women in US • #2 cause of death - African-American women aged 15-34 • 40-50% of US femicides by an intimate partner or ex-intimate partner (SHR analyses misclassifies many – Langford, ’98) • 67%-80% of intimate partner femicides were previously battered by their murderer
Pregnancy and Femicide • Femicide • Femicide accounted for 25% of the injury deaths of pregnant women in NY City (Dannenberg et al., 1995) • 13% of pregnancy related deaths were femicides in NC (Parsons & Harper, 1999) • 11 city study on intimate partner femicide, victims of femicide or attempted femicide were more likely to have been abused during pregnancy by the perpetrator than the comparison group of abuse women (McFarlane et al., 1999). • Study found a 3 fold increased risk of femicide, if the woman was abused during pregnancy
Pregnancy and Femicide • Femicide • Pregnancy in and of itself – is NOT a risk factor for femicide • Abuse during pregnancy is one of several risk factors for femicide/attempted femicide
Femicide • Femicide • Important to note other significant risk factors: • Previous threats to kill her • Partner/ex-partner unemployed and not looking for work • Partner/ex-partner is not the biological parent of a child living in the home • Woman is leaving the relationship and partner/ex-partner is controlling • Partner/ex-partner owns a gun
Kerry Repp Act-Oregon • Focus on women as victim of violence during pregnancy • Raise awareness of pregnancy as a dangerous time for some abused women • Training for health care professionals, coroners, law enforcement, judges related to lethality and pregnancy
Kerry Repp Act-Oregon • We need to know if femicide is the leading cause of maternal mortality in Oregon • Multidisciplinary Fatality Review System • State and County levels • Surveillance system of femicides in Oregon • Develop prevention and intervention strategies
Effects of IPV on Children • Anxiety reactions and post-traumatic stress symptoms, e.g., irritability, agitation, trouble concentrating, exaggerated startle response, intrusive, unwanted memories • School problems, e.g., declining grades, behavioral problems, truancy, suspensions, expulsions • More physical health problem than general population. • Worries about their mothers actual (e.g., battering) and potential (e.g., smoking, pregnancy) health hazards • Later, higher levels of violent behavior and arrests in children who have themselves been abused or neglected
Missed Opportunities • Few women report being asked about IPV at their health care visit (Glass et al., 2001) • 41% of women murdered by intimate or ex-intimate partner were seen at a health care agency for an injury or mental health issue in the year prior to murder (Sharps et al., 2001) • 20% of perpetrators of partner homicide were seen by a physician or mental health provider in year prior to murder (Sharps et al., 2001)
Public Health Problem Health Policy: Screening
Screening literature:“evidence insufficient” • Ramsey et al., British Medical Journal, 2002 • MacMillan & Wathen, Canadian Task Force on Preventive Health Care, JAMA 2003 • Anglin & Sachs., Acad Emerg Med, 2003 • Nelson et al., US Preventive Service Task Force, Annals Int Med., 2004
“Sometimes clinical judgement trumps Cochrane. Sometimes humanity trumps evidence. Or perhaps the type of evidence we demand for this kind of healing should be different from what we demand for the efficacy of anticoagulation in atrial fibrillation.” Lachs, Ann Intern Med 2004 p. 400
Who to screen? • EVERYONE! (Routine, Universal Screening) • Only 56% of women presenting to the ED because of intimate partner violence had an injury related diagnosis
How to Screen for IPV • Display visual information • How far does someone have to go in your setting before they know it is OK to talk about IPV? • Ask in private • Strategies to remove others from room prior to asking • Make it a safe process • Be nonjudgemental
What to ask? • Keep it simple! • How you ask more important than what you ask! • Have you been injured by a partner or ex-partner in the past year? • Is there anyone making you feel unsafe? • Has anyone made you have sex against your will?
Abuse Assessment Screen 1. Have you ever been emotionally or physically abused by your partner or someone important to you? 2. Within the last year, have you been hit, slapped, kicked, pushed or shoved, or otherwise physically hurt by your partner or ex-partner? If YES, by whom Number of times 3. Does your partner ever force you into sex? 4. Are you afraid of your partner or ex-partner? Heltin & McFarlane, 1986 Mark the area of any injury on body map.
Does Screening Identify Women at Risk? • Women with a positive partner violence screen are 9 times more likely (28% vs. 2%) to experience physical violence in the next three months (Koziol-McLain, 1999).
Document • Use her words • Name of perpetrator • History of abuse • Body Map, Photographs • Danger Assessment (Lethality, Suicide, Depression) • Interventions (Safety Plan) • Referrals (Hotline, Shelter, Legal, Police)
Assess Safety • Escalating violence (lethality) • Use or threat of weapon (gun, knife) • Lack of support and isolation • Recent separation from partner • Risk to children • Depression • Risk for suicide
Danger Assessment (Campbell, 2004) http://www.son.jhmi.edu • Developed in 1985 to increase battered women’s ability to take care of themselves (Self Care Agency; Orem ‘81, 92) • Interactive, uses calendar - aids recall plus women come to own conclusions - more persuasive & in adult learner/ strong woman/ survivor model • Intended as lethality risk instrument versus reassault (e.g. SARA, K-SID) - risk factors may overlap but not exactly the same
Danger Assessment • 20 items yes/no plus calendar • Shows pattern - frequency & severity of past year • Aids recall • Summative, no cutoff • 10 samples of 2251 battered women • Internal consistency = .60-.86; test-retest .89-.94 • Construct validity: convergent w/CTS & ISA (r = .55-.75); discriminant group
NATIONAL DOMESTIC VIOLENCE HOTLINE1-800 799-SAFE (7233)Family Violence Prevention Fundwww.endabuse.org