Download
1 / 18
190 likes | 709 Views
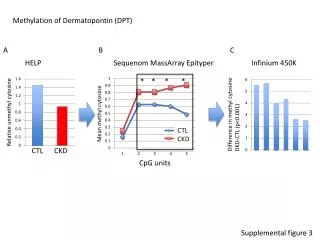
Managing Hypertension in CKD. 2012. Managing Hypertension in CKD. Why is the control of blood pressure important? What should our target be? What are the best medications?. Hypertension and CKD. Townsend Review

E N D
Managing Hypertension in CKD • Why is the control of blood pressure important? • What should our target be? • What are the best medications?
Hypertension and CKD • Townsend Review • Perera(1955) showed that although heart disease and stroke were commons findings, 18% of patients developed kidney function impairment in the course of untreated hypertension • Veterans Administration (VA) Cooperative Study Group on Antihypertensive Agents published in 1967 suggested that there were more cases of kidney failure in those treated with placebo as compared with those given active medication • KA Jamerson, Towsend RR; Advances in Chronic Kidney Disease, Vol 18, No 1 (January), 2011: pp 6-10
Hypertension and Progression of CKD Bakris et al. American Journal of Kidney Diseases, Vol 36, No 3 (September), 2000: pp 646-661
Pathophysiology • Brenner hypothesis (1981) – loss of autoregulation -> increase hyperfiltration -> increased Gp
Potential Factors • Endothelial damage • Podocyte injury • Local inflammatory factors • Tubuloepithelial protein reabsorption and oxidative stress • Increase matrix formation • Genetic factors • Angiotensin II
KDOQI Recommendations • The National Kidney Foundation clinical practice guidelines (1997)recommend a blood pressure goal of <130 mmHg systolic and <80 mmHg diastolic for all CKD patients. • Post-hoc analyses of the Modification of Diet in Renal Disease study indicate that lower blood pressure may provide long-term kidney protection in patients with nondiabetic kidney disease. Specifically a mean arterial pressure <92 mmHg (e.g. 120/80 mmHg) as compared to 102-107 mmHg (e.g. 140/90 mmHg) is associated with reduced risk for ESRD.
Other Guidelines • JNC and European Hypertension Society • 120/80 mm Hg is upper limit for optimal BP range in patients with CKD • Intervention should be initiated when BP > 130/80 mmHg
What Should The Target Be? • REIN-2 (ramapril) BP<130/80mmHg did not improve renal survival • AASK (ramapril, amlodipine, metoprolol) MAP of 102-107 did not improve renal survival but intensified BP control did slow progression in the subgroup of patients with proteinuria (>0.22Mg/mg creat)
What should our target be? • A Upadhyay et al Ann Int Med 2011:154:541 • No conclusive evidence favoring targets of less than 125/75 or 130/80 mm Hg v. 140/90 mmHg • Subgroups with proteinuria > 300-1000 mg/d or U P/C > 0.22g/g may benefit • Tx to lower targets requires greater vigilance to avoid adverse events and symptoms of hypotension
Proteinuria v. Non-proteinuria Meta-analysis of 11 studies. Jafar et al Ann Intern Med 2003;139:244
Combination Thearpies? • ACCOMPLISH (2010): ARB-CCB had superior BP control v ARB-diuretic. Losartan-amlodipine also had superior renal outocmes. • ONTARGET (Temilsartan + ramapril, 2008): showed inferior outcome • COOPERATE (trandolapril + losartan 2003): showed superior outcomes with the combination unlike ONTARGET
KDOQI • Dietary sodium restriction to no more than 2 grams daily is important. • Moderate alcohol intake, regular exercise, weight loss (>25 kg/M2), reduced saturated fat. • 1st line pharmacologic intervention: an ACE inhibitor or ARB in those with more than 200 mg protein/gram creatinine on a random urine. • Non-diabetics < 200 mg protein/gram creatinine, no specific first-line drug class is recommended. • After initial dosing a diuretic should be added. (Note: ACCOMPLISH might be suggestive that a CCB might be appropriate)
Key Articles • Managing kidney diease with blood pressure control. (2011)Wuhl E, F Schaefer. Nat. Rev. Nephrol. 7:434-444. • Upadhyay A, A Earley, SM Haynes, K Uhlig. Systematic Reviews: Blood pressure target in chronic kidney disease and proteinuria as an effect modifier. (2011) Ann Intern Med 154:541-548