Download

1 / 50
500 likes | 714 Views
A COMMON SENSE APPROACH TO CONTROLLING RISING HEALTH CARE COSTS. HMO. Major Medical Insurance. Fully-Insured. Point-of-Service. PPO Plans. INDEMNITY. CONSUMER DRIVEN HEALTH PLANS. BASIC PLANS. DEFINED CONTRIBUTION STRATEGY. Self-Funding. Are there Any New Ideas In Health Care?.

E N D
A COMMON SENSE APPROACH TO CONTROLLING RISING HEALTH CARE COSTS
HMO Major Medical Insurance Fully-Insured Point-of-Service PPO Plans INDEMNITY CONSUMER DRIVEN HEALTH PLANS BASIC PLANS DEFINED CONTRIBUTION STRATEGY Self-Funding
Are there Any New Ideas In Health Care? MSA PLAN Consumer Driven Indemnity HMO PPO POS
HEALTHCARE COVERAGE HISTORY • 1847 The first sickness insurance is offered in the US. The plan offers a scheduled payment for sickness or injury intended to replace income lost during sickness. • 1910 – Montgomery Ward & Co. Offers Employer Sponsored Group Insurance to Employees • 1917 – Railroad And Lumber Workers in NW offer pre-paid Medical Services (Predecessor of Blue Shield Insurance) • 1929 School Teachers Negotiate a Capitated Arrangement with Hospitals in Texas (Predecessor of Blue Cross Insurance) • 1930’s The first discounts were negotiated by an insurance company with doctors and hospitals (Predecessor to PPO’s) • 1940’s The majority of Blue Cross and Blue Shield Organizations Combine to form a single entity to insure both • 1950’s Scheduled Basic Coverage and Separate Major Medical Insurance Plans are the primary types of Insurance.
HEALTHCARE COVERAGE HISTORY • 1960’s Unions drive shift to First Dollar Office Coverage • 1968 – First Self-Funded Insurance Plan Offered by Firestone, Co. Coverage was Scheduled Basic Plus Major Medical, Employer Reimbursed Out of Pocket Expenses (Predecessor to Consumer Driven Plans) • 1970’s Indemnity Plans with Deductibles and Coinsurance are developed. • 1980’s PPO’s and EPO’s Developed and Gain National Acceptance • 1990’s HMO’s again Gain Popularity, PPO and Indemnity Enrollment Decrease • Mid 90s’ POS Plans Gain Popularity- HMO Enrollment Declines • 2000’s Defined Contribution, Consumer Driven Plans
Health Plan Enrollment by Plan Type, 1988-2003* *Source: KPF 2002,2003 Employer Sponsored Health Survey
WHAT HAPPENED??? • HIPAA • Employees Wanted More Choice- HMO Enrollment Decreased • HMO’s caused PPO’s to Lower Deductibles • PPO’s saturated the Market and Leverage Disappeared • Pharmaceutical Costs Rose Dramatically / Direct to Consumer
WHAT HAPPENED??? • Technological Advances Accelerated Other Treatment Costs • Hospitals and Doctors Normal Mark-up Became Dramatic • NOONE WILL ACCEPT THE RESPONSIBILITY! • Utilization Management / Case Management Changed
Who is to Blame? • Insurers Blame Pharmaceutical Manufacturers • Pharmaceutical Manufactures Blame HMO’s • HMO’s Blame Hospitals • Hospitals Blame Medicare and Medicaid • Doctors Blame Lawyers and Insurers • Everyone Blames Consumers
OUT WITH THE OLD & IN WITH THE NEW… And Improved???
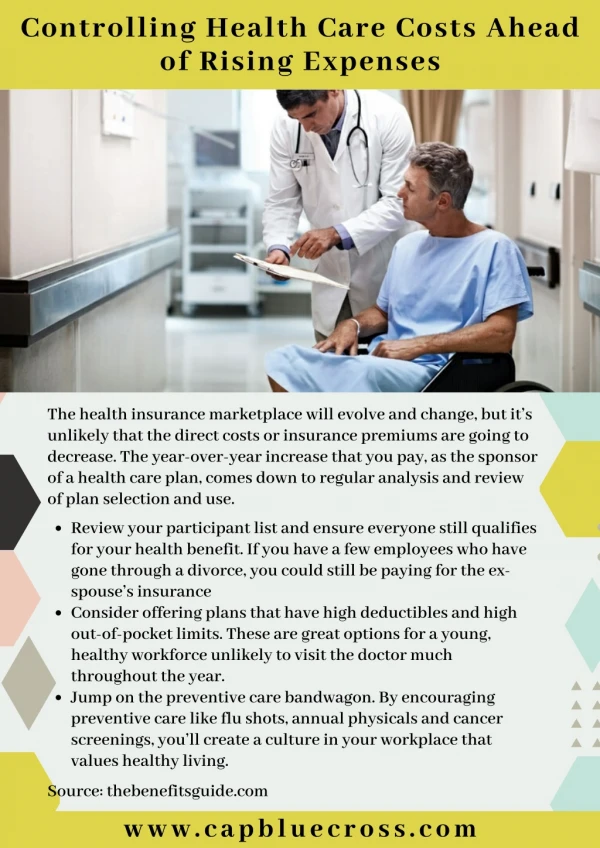
Out With The Old…In With The New… • Employers are Implementing New Plan Designs • - Higher Deductible Options with HRA’s • - More Choices
Out With The Old…In With The New… • 2. Employers are Migrating to Self-Funding
Out With The Old…In With The New… • Employers are Shifting More of the Premium to Employees. • - Defined Contribution Methodologies
Fully Insured Administration • The insurance company controls the “purse strings”. • The insurance company typically employs the utilization management nurse as well as case managers and physician consultants. • All parties make decisions based on the coverage as defined by the certificate of insurance.
SELF-FUNDED ADMINISTRATION • The employer controls the “purse strings” • The TPA is contracted by the employer to ensure good stewardship of plan assets. • TPA’s typically contract with vendors for Utilization and Case Management. • Plan provisions for Utilization and Case Management Mirror the Fully Insured Plans.
PLAN BENEFIT INTERPRETATION • Utilization Management / Case Management Vendors Are Medical Care Professionals, first. • Interpretation of Plan Benefits Remains the Responsibility of the TPA & Employer • Typically, UM / CM recommendations are not for the financial interest of the plan.
PLAN BENEFIT INTERPRETATION • TPA’s hire UM/CM vendors for their expertise, and rely on their recommendations. • UM / CM vendors do not interpret benefits
SENTINEL CLAIM REVIEW SOLUTION? • Work in Concert with UM / Case Manager to Offer Benefit Interpretation. • Identify Opportunities for Savings – Direct Care to More Appropriate Provider or Setting.
SENTINEL CLAIM REVIEW SOLUTION? • Provide Pertinent Plan Benefit Interpretations. • Negotiate Discounts When Possible.
HOSPITAL BILLING STRATEGIES • No two facilities bill alike. • Medicare Rules dictate Hospital Billing Practices. • Medicare Rules accept services not covered by their coding guidelines.
HOSPITAL BILLING STRATEGIES • Facilities determine new ways to take advantage of loop-holes in Medicare rules to achieve necessary revenue on Medicare Claimants. • Medicare Rules dictate Hospital Billing Practices.
SENTINEL CLAIM REVIEW SOLUTION? • Comprehensive Hospital Auditing and Determination of Coverage Based on Normal Billing Practices. • Common Sense Approach to Hospital Charge Reimbursements.
SENTINEL CLAIM REVIEW SOLUTION? • Negotiation of Non-Discounted Admissions. • Patient Education and Follow-up Services for the Employer.
Formula For Savings • Research, Research, Research. • Bridge the gap between UM/CM interpretation and plan benefits interpretation. • Understand costs of care and billing trends
Formula For Savings • Watch and document industry billing and treatment trends. • Hold providers accountable for their billing practices, and charges. • Leverage Negotiations Where Possible Through Retrospective Audits.
Formula For Savings • Find Ways to Reduce Costs on Individual Treatments – In Concert With Physicians. • Proactively Pursue Alternative Ways to Achieve the Same Results at Less Cost. • Educate the Patient, Employer and Provider, Whenever Possible.
Renal Dialysis Treatment Renal Dialysis Treatment Consists of: • The Procedure of Blood Filtration • The Routine Infusion of Drugs • Conditioning of the Quality of the Blood With Fortifying Drugs and Supplements
COST ANALYSIS Dialysis Expected Costs are Approximately: $500 per week for Filtration $100 per week for Misc. Admin Costs $14.40 per unit for Anemia Drug, Procrit, times 120 units per week ($1,728)
Typical Issues Affecting Costs • The Majority of ESRD Patients are Medicare Primary. • Medicare Reimbursement for Drugs And Supplies is Usually Below Cost • Physicians Mark-up Supplies To Compensate for Losses. • Mark-ups on Procrit May Exceed 600%
Annualized Cost Comparison • Dialysis Actual Costs Per Week: $2,328, or $121,056 per year. • Marked-up, costs may exceed $10,968, or $570,336.
Typical Plan Allowance • Usual and Customary Typically Allows the Average Charge Billed in a Region. If 600% is the Average Mark-up, the entire $10,968 per week may be allowed. • PPO’s generally do not allow negotiation of charges. Most networks require reimbursement at a percentage of billed charges. So only a small savings would be achieved.
Sentinel Response • We Attempt Negotiation of the High Drug Mark-up to a Small Percentage of Actual Pharmacy Costs. • If the Provider Refuses, We Offer to Have the Drug Delivered to the Provider at Plan Cost- For Each Treatment. • We Contact All Competitors to This Provider to Determine if Charges are Fair and Equitable.
Sentinel Response • Our Average discount is 30% off Drug Charges, over and above any other discount. • Based on this example, total savings would average $161,740.80.
Hospital Pass Through Devices Hospital Normal Average Mark-up is 175% to 250% • Most supplies and Drugs are Hospital Inventory Items. Hospitals Mark up Inventory to cover facility costs, staff and Medicare/Medicaid Shortfalls. • Some Items are Pass Through Devices – Which Means the Hospital Does not Keep them In Inventory.
Hospital Pass Through Devices Pass Through Devices Include such Items as take home medical equipment, drugs and such devices as internal pacemakers. The normal average mark-up for Pass Through Devices is 6% over Cost.
Typical Pacemaker Charge The Average Standard Pacemaker Costs $25-30,000. A New Generation Pacemaker with Ventricular Defibrillator May Cost $45,000. A Ventricular Assist Device (VAD) May run $70,000.
Typical Pacemaker Charge At 106% of cost, the average mark-up would be: $1500 to 1800 for a Standard Device $2700 for a Ventricular Defibrillator $4200 for a VAD While this seems High, the device Mark-up is generally accepted. Medicare pays 100% of the pass through cost for each device.
Typical Pacemaker Charge Some providers carry the same mark-up for inventory supplies and pass-through devices. At 175% of cost, the average mark-up would be: $18,750 to $22,500 for a Standard Device $33,750 for a Ventricular Defibrillator $52,500 for a VAD
Sentinel Response • We Attempt Negotiation of the pass through device to a Percentage of Hospital Costs. • We Contact All Competitors to This Provider to Determine if Charges are Fair and Equitable.
Sentinel Response • Our Average discount is to 112%, over cost. • Based on this example, total savings would average $15,750 to $44,100.
Sentinel Claim Review Provides Audit/ Interpretation Services For: Employers Third Party Administrators Insurance Companies We also Offer Claim Audit / Cost Consulting for: Reinsurance Carriers Managing General Underwriters And Fiscal Intermediaries for Medicare/Medicaid
Sentinel Claim Review 5560 W. Grande Market Drive Appleton, WI 54913 Phone: (920) 968-4482