Download
1 / 43
430 likes | 566 Views
Practice-based Quality Improvement Session 2 PCFDP November 12, 2010 Stephanie Berkson , MPA Sally Kraft, MD, MPH. Session Objectives. Understand the basic model of improvement: FOCUS PDCA Be able to lead an improvement team through each step in FOCUS

E N D
Practice-based Quality ImprovementSession 2PCFDPNovember 12, 2010 Stephanie Berkson, MPA Sally Kraft, MD, MPH
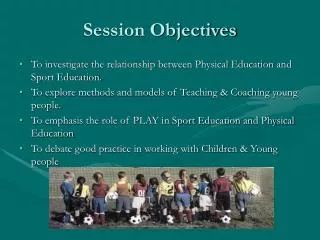
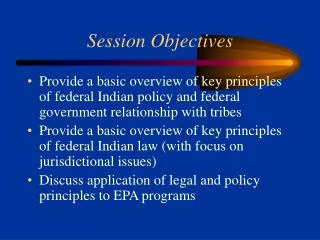
Session Objectives • Understand the basic model of improvement: FOCUS PDCA • Be able to lead an improvement team through each step in FOCUS • Be able to write a specific AIM statement
Imperatives for Change • Unexplained Variation in Quality and Costs • Dartmouth Atlas for Health Care http://www.dartmouthatlas.org/ • Medical errors • 2000 IOM To Err is Human: 98,000 lives lost/year due to medical errors • High costs • 17% of GDP • 2005 IOM Building a Better Delivery System: 30-40 cents of every health care dollar is spent on waste (overuse, underuse, misuse)
Imperatives for Change • Poor outcomes • US spends over twice as much per capita on health as compared to other industrialized nations but ranks last in number of preventable deaths • Disparities • 2002: Life expectancy at birth for a white male = 75 years, for a black male = 69 years. Even when correcting for education and income, African Americans have worse health outcomes compared to white Americans. • Uninsured • 15 % uninsured, 30% underinsured
Goals for Improving the US Healthcare System • The Triple Aim • Improve the patient care experience (quality of care, access, coordination) • Improve the health of the population • Lower costs without causing harm
Goals for Improving the Quality of Healthcare • STEEEP • Safety • Timeliness • Equity • Efficiency • Effectiveness • Patient- and family-centeredness • 2001 IOM Crossing the Quality Chasm
Focus on Process Improvement • Exercise: • At each table, identify 3 health care processes that you do exactly the same every single time you perform the activity.
Improving Quality:Focus on Process • Example: Drawing blood cultures • Despite the fact that you are drawing blood cultures on different patients in different settings, you always draw cultures the same way. • Structure Process Outcome
Dimensions of Care • Structure: • The capacity to provide care reflected in the quantity, type, and qualifications of individuals and facilities. • Good structure does not guarantee high quality • Examples: Physician certification, nurse-to-bed ratio • Process: • What is done when providing care. Appropriateness (doing the right thing) and skillfulness • Example: inserting a central line, screening all eligible patients for breast cancer • Outcome: • Effects of health care on a patient’s health status and satisfaction
Eliminating Central Line Infections in Michigan Pronovost NEJM 2006; 355: 2725
Pilot Site Go-Live w/ Steps 1&2 Wave 1 MDs Go-Live w/ Steps 1&2
Standardized Processes for Handling Phone Calls Since Jan 2008, abandon-ment rate decreased from 13% to 1.3% !! Dropping Press Ganey scores until Dec 2007, then high score of 100 in June 2008! OA Phase II Phase I UWMF Clinics
Basic Model for Improvement • What are we trying to fix? • How will we know if we have improved? • What changes can we make that will lead to improvement?
Basic Model for Improvement • What are we trying to fix? • FOCUS • (Find a problem, Organize the improvement team, Clarify the current situation, Understand the causes of variation and poor quality, Select solutions to test) • How will we know if we have improved? • DATA • What changes can we make that will lead to improvement? • PDCA • (Plan-Do-Check-Act)
Find a Process to Improve • Review performance data • Ask your clinic team • Ask your patients • Evaluate your practice, the 5 P’s • Know your purpose • Know your patients • Know your professionals • Know your processes • Know your patterns
Practice Process Assessment: A Tool to Understand Your Processes Core Ambulatory Practice Process Assessment Name:____________________________________ Date: ____________________ Rate each of the following practice support processes by placing a checkmark under the heading that most closely matches your understanding of the process for your clinic. Also mark it if the process is a source of patient complaints. Full template is provided in your handouts
Global Aim • After assessing your practice and reviewing performance data, identify what aspect of the practice you will improve. • Exercise: You are reviewing your practice assessment and organizational performance data on telephone performance at your clinic. Write a global aim statement using the template provided.
Phone abandonment rates were higher than organizational goal (3 - 5%) Average abandonment rates June 2007 to Dec 2007: 10% - Clinic 4% - Organi-zation Low patient and provider satisfaction with Communications Center performance OA Opened new OA neighborhood UWMF Clinics OA Opened new OA neighborhood
Organize a Team • Include the people who do the work on the improvement team • Challenges in working with a team • Running effective team meetings • Stakeholders v. team members
Effective Meetings • Running an effective meeting is a skill and requires practice and hard work • 2.Tips for success: • Prepare: create an agenda, state the objectives for the meeting • Make sure the right people are included • Assign roles: Facilitator, Time keeper, Recorder • Clearly state “next steps” and assign accountability • Evaluate the meeting
Stakeholder Analysis • Used by the change team to create an enrollment and involvement strategy for each group • Analysis provides • Who is affected • How they are affected • How critical they are in the process • Who should be contacted
Clarify the Current SituationUnderstand the Causes of Variation and Poor Performance • Work with the entire improvement team • Use brainstorming techniques to understand the current state and uncover reasons for defects • Collect data to improve your understanding of the current situation • Review the literature, identify best practices
What is it? Identifies the “drivers” of the end product Why would you use it? Shows all activities that contribute to the end product Places activities into “buckets” to help focus your improvement work When would you use it? At the beginning, when you have an end product you want to improve Cause & Effect Diagram
Phone abandonment rates were higher than organizational goal (3 - 5%) Average abandonment rates June 2007 to Dec 2007: 10% - Clinic 4% - Organi-zation Low patient and provider satisfaction with Communications Center performance Create a Cause and Effect Diagram to Explain this Poor Performance OA Opened new OA neighborhood UWMF Clinics OA Opened new OA neighborhood
Data Collection to Clarify and Understandthe Problem • External sources of data are typically not appropriate or readily available • Internally collected data is ideal for improvement work • Qualitative data • Quantitative data • Data needs to be valid, feasible, and consistent • Exercise: create a data collection sheet to identify the causes of the high phone abandonment rate at the clinic
Definition Illustration of steps in a process using symbols and arrows Purpose Understand existing processes Identify non-value added steps Clarify complex processes Identify improvement opportunities Generate alignment and agreement Train new staff Process Map Basics
Select Solutions to Test • Select one specific solution to test that: • addresses a cause of the problem • is within the scope of control of your team • has key stakeholders’ support • 2. Develop a SMART aim statement • Specific • Measurable • Agreed upon and actionable • Relevant • Time-bound
SMART AIM Statement • I/We will achieve improvement in • [Process] • by (increasing/decreasing/improving) • [Key aspect(s) of process performance] • by [Amount] • within [Time Frame] • focusing on • [Actions and strategies for change]
Goal Reduce clinic telephone abandonment rate to 3% or below by August 2008 Defined Project Metrics Quantitative – Abandonment rate (AR), call volumes Qualitative – Patient and provider satisfaction with access to reaching clinic by phone OA Abandonment Rate Goal
We’ll focus on applying the PDCA process in Session 3. • Skills we will practice at the Jan session: • Developing and implementing an action plan • Collecting improvement data; measuring processes and outcomes • Assessing strategies for sustaining improvements