Download
1 / 48
670 likes | 1.38k Views
Fat-Soluble Vitamin Deficiencies. Andrew Ukleja, M.D., C.N.S.P. Assistant Professor of Medicine Director of Nutrition Support Team Department of Gastroenterology Cleveland Clinic

E N D
Fat-Soluble Vitamin Deficiencies Andrew Ukleja, M.D., C.N.S.P. Assistant Professor of Medicine Director of Nutrition Support Team Department of Gastroenterology Cleveland Clinic Weston, FL
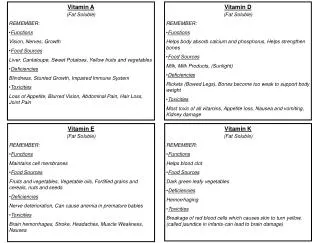
Objectives • To review • Functions of fat-soluble vitamins (A,D,E,K) • Symptoms and signs of vitamin deficiencies • Treatment of vitamin deficiencies
Vitamin Deficiencies • It takes months to years for fat soluble vitamin deficiencies to develop because of relatively large stores Result of • Decreased intake • Decreased absorption • Increased utilization • Increased loss
Vitamin A RETINOL RETINAL (RETINALDEHYDE) RETINOIC ACID BETA-CAROTENE
Metabolism of Vitamin A • Absorption: proximal small bowel • Transported by chylomicrons (retinyl ester + retinol) • Stored in liver (esters + CRBP [cellular retinol binding protein]) • Stellate cells 80-90% • Hepatocytes 10-20% • Released into plasma as retinol + RBP (bound to prealbumin) • From diet: 50% stored in the liver 20% excreted in feces (from bile) 17% excreted in urine 10% not absorbed 3% CO2
Functions of Vitamin A • Vision • Phototransduction • Regulation of gene expression • Immunity • Maintenance of the integrity of skin, and mucosal cells (airways, digestive and urinary tract) • Differentiation of WBC, activation of T-lymphocytes • Growth and development • Red blood cell production • Stem cells differentiation into red blood cells • Mobilization of iron from storage sites
Vitamin A and Vision Photoreceptor (Rod) Cell Retinal Pigment Epithelium Capillary 11-cis-retinal 11-cis-retinal LIGHT Rhodopsin 11-cis-retinol Neuronal signaling Opsin Opsin + All-trans-retinyl ester all-trans-retinal VISION All-trans-retinol all-trans-retinol All-trans-retinol
Dietary Sources of Vitamin A • Animal foods: Liver, fish oil, kidney, egg yolk, butter • Plants: Carrots, dark green leafy vegetables (beta-carotene), spinach, broccoli, sweet potatoes • RDA: 700-900 mcg 1mcg of retinol=3.33 IU of vit. A
Vitamin A Deficiency • Ancient Egyptians recognized that night blindness could be treated by consumption of liver • 3rd most common nutritional deficiency in the world • Night blindness, complete blindness, and xerophthalmia common in malnourished children in Asia, Africa, and South America • Vitamin A deficiency is rarely seen in the United States
Causes of Vitamin A Deficiency • Inadequate intake (strict vegetarian diet) • Fat malabsorption • Crohn's ileitis • Pancreatic insufficiency • Cystic fibrosis • Cholestatic liver disease • Severely limited protein intake • Vit. A carried by RBP
Vitamin A Deficiency Clinical Manifestations • Night blindness • Bitot's spots - Abnormal squamous cell proliferation and keratinization of the conjunctiva Xerophtalmia 3. Irreversible eye conditions: Xerosis Corneal perforation Keratomalacia Punctate keratopathy
Vitamin A Deficiency • Dermatologic manifestations: • Follicular hyperkeratosis (Dry, rough, scaly skin) • Destruction of hair follicles • Impairment of the humoral and cell mediated immune response • direct and indirect effects on phagocytes / T cells: incidence of respiratory disease/diarrhea rate of mortality from infections in children
Assessment of Vitamin A Status • Biochemical: • Deficiency: serum vit. A level <0.35mcmol/L (<10mcg/dl) measured by HPLC • 50% increase in RDR assay - change in serum retinol level before and 5 hrs after oral dose of 450-1000 mcg of retinyl ester • Histologic (conjunctival impression cytology) • Physiologic (measurement of dark adaptation) • Dietary
Assessment of Vitamin A Status • Serum retinol levels vary widely • Serum retinol level is not influenced by dietary intake • in serum retinol by 20 % after a challenge dose indicates limited hepatic stores • Healthy: Ratio of plasma retinol / RBP =1
Supplementation of Vitamin A • Tolerable upper level for adult: 10,000 IU/d (3 mg/d) • MVI supplement - 5,000 IU (1.5 mg) of vitamin A • Retinol intake of 5,000 IU/day have been associated with risk of osteoporosis in older adults • Rx of Vit. A deficiency: 30 mg of retinol palmitate, single IM injection (children)
Vitamin D • Vitamin D and its metabolites play an important role in calcium homeostasis and bone metabolism • Vitamin D deficiency (referred to "rickets“) was first described in the mid 1600s by Whistler and Glisson • Severe bone-deforming disease: enlargement of epiphyses of long bones, bowing of the legs, bending of the spine and toneless muscles
Vitamin D Metabolism ultraviolet light P450 Intestinal absorption
Functions of Vitamin D Low Calcium
Functions of Vitamin D • Calcium homeostasis • Immune response • IL4 production, T cell activity • Cell growth and differentiation • Apoptosis • Protects against peroxidation
Sources of Vitamin D • Vitamin D is found naturally in very few foods • Dietary source: fatty fish (mackerel, salmon, sardines), cod-liver oil, eggs yolks • Fortified milk (vitamin D2/D3), cereals and bread products, orange juice • Infant formula is fortified with vit. D (400 IU per quart)
Causes of Vitamin D Deficiency • Impaired availability of vitamin D • Inadequate intake of vitamin D • Fat malabsorption • Lack of photoisomerization • Impaired hydroxylation to 25-hydroxy-vitamin D • liver disease • Impaired production of 1,25(OH)2-vitamin D • kidney disease
Risk Factors for Vitamin D Deficiency • Exclusively breast fed infants - human milk 25 IU/L of vit. D • Dark skin - vit. D synthesis with exposure to sunlight • Fat malabsorption - absorption of vit. D • Elderly - synthesis of vit. D in the skin + stay indoors • Institutionalized adults • Obesity - vit. D deposited in body fat stores
Findings in Vitamin D Deficiency • intestinal absorption of calcium and phosphorus • Hypocalcemia • Hypophosphatemia • Phosphaturia • Secondary hyperparathyroidism (bone resorption) • Demineralization of bones • Osteoporosis/ostoemalacia in adults • Rickets in children • Muscle pain/weakness
Vitamin D Deficiency Children Rickets • Failure of bone mineralization in infants and children • Delayed closure of the fontanels (soft spots) in the skull • Deformed rib cage in infants • Seizures from hypocalcemia
Assessing of Vitamin D Status • Serum 25(OH)D3 level • Normal level 75-125 nmol/L • Severe deficiency < 20-25 nmol/L • Serum 1,25(OH)2 D level • Undetectable in severe deficiency • PTH level • BMD (DEXA scan)
Vitamin D Supplements • RDI: 400 IU (0.01 mg of vit. D3) • Multivitamin supplements with vit. D • Children 200 IU (5 mcg) • Adults 400 IU (10 mcg) • Vitamin D (D3) supplement: 400-1,000 IU • Older adults (>65 years) + those with minimal sun exposure should take 800 IU/d of vit. D
Treatment of Vitamin D Deficiency • Osteomalacia: • Vit D3 orally: 4,000-8,000 IU/d (0.1-0.2 mg) • If malabsorption up to 50,000 IU/d orally • Monitor 25-OH-vit. D levels q 3-4 weeks until normal • MVI IV form contains 200 IU of vit. D2 • Sun exposure: 10-15 minutes of on the arms and legs at least x3 weekly
Vitamin E • The name tocopherol came from the Greek word of "toc" (child) and "phero" (to bring forth) to describe its role as an essential dietary substance in normal fetal and childhood development
Functions of Vitamin E • A free radical scavenger, protects PUFA (a structural component of the cell membranes) from peroxidation • Inhibits activity of protein kinase C • Affects the expression and activity of immune and inflammatory cells • Inhibits platelet aggregation and enhances vasodilation
Vitamin E • Suboptimal intake of vit. E is relatively common in the U.S. • Food source: vegetable oils (olive, sunflower, safflower), nuts and seeds, whole grains, green leafy vegetables • Vit. E is destroyed by heat • The RDA for vitamin E • Women 8 mg/d • Men 10 mg/d
Metabolism of Vitamin E • Intestine: Pancreatic esterases brake down tocopheryl-ester bonds between vitamin E and fatty acids • Liver: alpha-tocopherol is packaged within VLDL molecules • Blood: Transported by A-tocopherol transfer protein • Vit. E is stored in adipose tissue (90%)
Causes of Vitamin E Deficiency • Severe malnutrition / cirrhosis • Genetic defects affecting the alpha-tocopherol transfer protein/abetalipoptoteinemia • Fat malabsorption syndromes • Pancreatic insufficiency • Celiac disease • Regional enteritis • Small bowel bacterial overgrowth • Cystic fibrosis • Cholestatic liver disease • Postgastrectomy syndrome
Vitamin E Deficiency • Vitamin E deficiency is uncommon due to the abundance of tocopherols in our diet • Divided to: • Subclinical (low serum tocopherol level) • Clinically evident • Consequences of vit. E deficiency • Neuromuscular disorders • Hemolysis
Symptoms of Vitamin E Deficiency Neurological: • Spinocerebellar ataxia • Peripheral neuropathy • Muscle weakness/skeletal myopathy • Pigmented retinopathy (retinitis pigmentosa) • Hematologic: • Hemolysis- red blood cell life span • Hemolytic anemia common with vitamin E deficiency in premature infants
Evaluation of Vitamin E Status • Serum total alfa-tocopherol concentration • Normal level > 0.5 mg/dL • Tocopherol isomers (by HPLC) • Peroxide hemolysis test (2% hydrogen peroxide) • Tocopherol/total lipids ratio • Normal > 0.8mg/g
Vitamin E Supplementation • Tolerable upper intake: 1,500 IU/d (1,000 mg/d) • Side effects: impaired blood clotting/ risk of hemorrhage seen in adults with vit. E < 2,000 mg/d • Large oral supplements of vit. E have been associated with • Necrotizing enterocolitis in infants • Higher mortality due to hemorrhagic strokes in adults • Impaired absorption of vitamins A and K seen with large vitamin E supplements in animals
Vitamin K • The "K" is derived from the German word "koagulation“ • Two forms of vitamin K • Vitamin K1 (phylloquinone) - dietary from plants • Vitamin K2 (menaquinone) - synthesized by gut micro-flora • Vitamin K is essential for the functioning of several proteins involved in blood clotting
Metabolism of Vitamin K • Vitamin K is absorbed in the distal small intestine • Dietary vitamin K is protein-bound and requires liberation by proteolysis (pancreatic enzymes) • Bile salts solubilize vitamin K into micelles for absorption into chylomicrons (transport via portal circulation to the liver) • Microorganisms of the colon and distal ileum can synthesize absorbable vitamin K
Functions of Vitamin K • A major role in coagulation pathways • Essential for activity of carboxylase enzymes responsible for carboxylation of glutamate to gamma-carboxyglutamate (liver) • Clotting factors – prothrombin, factors VII, IX, X • Anticoagulant proteins C, S • Osteocalcin • Hydroxylation of osteocalcin (bone matrix)
Vitamin K • Dietary source • Liver • Oils (soy, canola, olive) • Green leafy vegetables (spinach, broccoli) • Current DV for vitamin K: 65-80 mcg/d
Vitamin K Deficiency • Vitamin K deficiency is rare in adult • Factors protecting from vit. K deficiency • Wide distribution of vit. K in plants and animal tissue • Production of vit. K by gut micro-flora • Recycling of vitamin K • vitamin K levels seen with prolonged fasting or starvation • Acquired deficiency can occur secondary to • Long-term use of antibiotics
Causes of Vitamin K Deficiency • TPN (no dietary intake) • Rx: Vit.K 1 mg/week • Malabsorption • Rx: vit.K 1-2mg/d p.o. • Biliary obstruction • Liver disease • Drugs: • Coumarins, salicylates, antibiotics, vit. A&E
Signs and Symptoms of Vitamin K Deficiency • Mucosal bleeding • Easy bruisability • Splinter hemorrhages • Melena • Hematuria
Vitamin K DeficiencyHemorrhagic Disease of the Newborn • Causes: • Poor transfer of lipids via placenta • Immature liver • Sterile GI tract • Breast milk low in vit. K • Infants at risk • Diarrhea • Malabsorption • CF • Cholestasis • TPN Rx: 1mg I.M. of vit. K
Determination of Vitamin K Status Measurements • Levels of vitamin K-dependent factors (prothrombin, factors VII, IX, X, protein C) • Vitamin deficiency: factor levels < 50% of normal • Plasma Vit. K level (normal 0.2-1.0 ng/ml) • Plasma Des-gamma-carboxyprothrombin (DCP) • Normal subjects DCP=0 • Vitamin K deficiency DCP
Vitamin K • Treatment of coagulopathy • Vitamin K in doses 1-25 mg orally, IM, IV, SC • Vitamin K IV can cause severe anaphylactic-type reaction • Prevention of hemorrhagic disease of the newborn • Vitamin K 0.5-1 mg IM at birth