Download
1 / 128
1.33k likes | 1.38k Views
NERVOUS SYSTEM DISORDERS. And Associated Nursing Care. Conciousness Increased Intracranial Pressure (ICP) Head Injury Degenerative and Autoimmune Nervous System Disorders. Consciousness. Consciousness.

E N D
NERVOUS SYSTEM DISORDERS And Associated Nursing Care
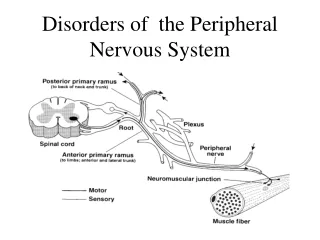
Conciousness • Increased Intracranial Pressure (ICP) • Head Injury • Degenerative and Autoimmune Nervous System Disorders
Consciousness Is a condition in which the person is aware of self and the environment and is able to respond appropriately to stimuli (McLeaod, 2004). Two components: • Arousal: (or awakeness) reflects activity of RAS, thalmus and upper brain stem. • Content: cognitive mental functions reflects cerebral cortex activity (thought processes, memory, perception, problem solving, & emotion)
Altered Consciousness • Definition: condition of being less responsive to and aware of environmental stimuli (Smeltzer & Bare, 2004). Unconsciousness • Definition: physiological state in which the client is unresponsive to sensory stimuli and lacks awareness of self and the environment (Hickey, 2003)
Unconsciousness • Can be brief, lasting a few second to a few hours or longer. • To produce unconsciousness a disorder must: • Disrupt the RAS which extends up to the thalmus. • Significantly disrupt the function of both cerebral hemispheres • Metabolically depress overall brain function
Coma Coma is a prolonged state of unconsciousness in which the client is unaware of self or the environment for sustained periods of time from hours to months. (Hickey, 2003) Because of: -disorders that affect BOTH cerebral hemispheres - disorders that affect any part of the RAS - direct compression on parts responsible for conciousness ie: hemorrhage, tumors - metabolic disorders (hypoglycemia, hypoxia) - toxins ** Duration of coma is associated with mortality & outcome****
Major Causes and manifestations of Altered Consciousness Reduction in level of consciousness may be caused by extracranial or intracranial causes.
Intracranial Causes Supratentorial lesions (above the cerebellum) • A lesion must affect the cerebral hemispheres directly and widely to cause diffuse bilateral hemispheric dysfunction and subsequent coma (Hickey, 2003) Infratentorial Disorders Involve cerebellum and brain stem • Cause sudden LOC • Usually produce: • Early coma - Abnormal respiratory patterns - Oculorvestibulary abnormalities - Pupillary changes
Extracranial Causes: Metabolic Disorders or Toxins • Usually produces confusion first • Findings are symmetrical or bilateral • Physical symptoms include tremors, asterexis,, myoclonus & seizures. • Pupillary response is normal unless related to drug overdose.
Examples • Hypoxemia • Hypercapnia/acidosis • Hypotension • Blood sugar alterations (DKA, hypoglycemic coma) • Liver dysfunction • Fluid/electrolyte disorders • Multiorgan dysfunction • Drug effects
Psychogenic Coma • Although rare, pychogenic disorders such as hysteria, catatonia, and severe depression can cause alterations in LOC • Despite outward appearances the person is physiologically awake.
Assessment • Glasgow Coma Scale • Mini-mental • Diagnostic Tests • CT and MRI • Lumbar Puncture • EEG • Laboratory Tests • Tests for Abnormal Reflexes • Oculocephalic Reflex Response • Oculovestibular Reflex Response
The Glasgow Coma Scale The Glasgow Coma Scale (GCS) is a universally used neurological assessment tool to assess degree of consciousness impairment. CGS measures eye, verbal, and motor response. It is an excellent scale to measure arousal. It is less helpful related to content measurement. Know the difference b/t content & arousal
GLASGOW COMA SCALE SCORE (GCS) Eyes 1 Closed at all times 2 Opens to pain 3 Opens to voice command 4 Open spontaneously Motor 1 No response 2 Extension (decerebrate) 3 Flexion posturing (decorticate) 4 Flexion withdrawal 5 Localizes painful stimulus 6 Obeys commands Verbal 1 No response 2 Incomprehensible sounds 3 Inappropriate words 4 Disoriented and converses 5 Oriented and converses 15 (top score) A score of 10 or less indicates a need for emergency attention A score less than 7 is interpreted as coma
*Level of consciousness is the single most important indicator of neurological function and change* * Important!
CONTENT Besides orientation to time, place and person the following cognitive abilities should also be assessed: • Attention and vigilance • Memory – short, intermediate, long term • Language – understanding of spoken and written word • General fund of information • Construction ability • Sequencing activities • Problem solving • Abstraction • Insight and judgment The Mini Mental Status Exam is an example of a test for cognitive function. (Used on GARU).
Diagnostic Tests • CT or MRI: data on structural causes such as tumor or hemmorhage. -Metabolic – will be unremarkable • LP: infection or bleeding (cloudy or bloody) • EEG: structural or metabolic, seizure activity • Lab tests: LFTs, kidney function, glucose levels, toxicology, ABGS
Diagnostic Tests for Abnormal Reflexes • Oculocephalic reflex response – abnormal if eyes remain in fixed position when head turned • Oculovestibular reflex response – absence of eye movement when water instilled in ear = brain death
Medical Management: goal is to preserve brain function & prevent further damage • Determine Level of Involvement • Reverse Common Causes of Coma • Prevent Complications
Nursing Diagnoses • Altered Tissue Perfusion • Risk for Suffocation/Aspiration • Altered Oral Mucous Membranes • Risk for Impaired Skin Integrity • Risk for Contractures • Altered Nutrition: Less than Body Requirements • Fluid volume deficit • Risk for Injury • Altered family processes
Maintaining the airway Protecting the patient Fluid balance Mouth care, skin and joint integrity Corneal integrity Thermoregulation Nursing management
Nursing Assessment: Brain Injury • ABCDs • Maintaining airway • History if possible • Determine LOC, ability to respond to verbal commands, reactions to tactile stimuli, status of reflexes. • Glasgow Coma scale • Fluid and electrolyte balance • Monitoring/managing potential complications
Intracranial pressure • ICP is the pressure exerted by the brain tissue, CSF, and cerebral blood within the intracranial vault.
There is a delicate balance that exists between the volume of the intracranial contents within this rigid compartment (80% brain tissue, 10% blood, 10%CSF) • The normal ICP is 0-15 mmHg (15 is the upper limit). • Pressures over 20mm Hg represent severely increased ICP,which seriously impairs cerebral perfusion.
Important Parameters Affecting ICP • Cerebral perfusion pressure (CPP) • Cerebral blood volume (CBV) • Cerebral blood flow (CBF)
Cerebral perfusion pressure (CPP)is the amount of blood flow (pressure gradient ) from the systemic circulation that is required to provide adequate oxygen and glucose for brain metabolism. • It is the difference between mean arterial pressure (MAP) and ICP. CPP = MAP – ICP • Mean arterial pressure (MAP)represents the average pressure during the cardiac cycle. Calculate by: systolic pressure + 2 X diastolic divided by 3. Example BP 70/34. MAP= 46
Cerebral blood volume (CBV) is dependent on cerebral blood flow (CBF). • If CBF increases, so does CBV. CBF depends upon cerebral perfusion pressure (CPP). When MAP & ICP are equal there is no CPP & blood flow stops! )
Maintenance of ICP Autoregulation is the compensatory changes in the diameter of the intracranial blood vessels designed to maintain a constant blood flow during changes in systemic arterial pressure (cerebral perfusion pressure).
Critical point may be reached when either: • the ICP is greater than 30 to 35 mm Hg • systemic blood pressure is less than 60 mm Hg • Systemic BP greater than 160 mm Hg. Autoregulation is lost with increasing ICP. After this the CBF will vary passively with systemic blood pressure.
The Munro-Kellie Hypothesis Know this! The Munro-Kellie Hypothesis states that a change in volume of any of the normal components (brain, cerebral blood volume and cerebrospinal fluid) of the intracranial vault must be accompanied by a reciprocal change in one or more of the other components. If this reciprocal change is not accomplished the result is an increase in intracranial pressure (ICP).
How does the body compensate for changes in ICP? 1. Compliance • Displacement of CSF into the spinal subarachnoid space • Increased absorption of CSF • Decreased secretion of CSF
Compensatory mechanisms cont’d 2. Reduction of blood volume in the brain. • Venous blood may be shunted to allow more room for expansion. • As this ability decreases, the venous pressure increases, & CBV and ICP rise • This stage of compensation alters cerebral metabolism, eventually leading to brain tissue hypoxia and areas of ischemia.
Compensatory mechanisms cont’d 3. Herniation displacement of brain tissue. Most lethalstage of compensation. Process often results in death from brain stem compression. Always an emergency!
Results! • Compression • Laceration • Vascular compromise • Necrosis of structures • Blocked flow CSF • Brain compression and death
Common Causes • Increases in tissue volume • Space occupying lesions: brain tumor, abscess, hemorrhage, • Cerebral edema: infarction, interstitial edema, infection, metab0olic disorders, toxins, electrolyte imbalances • Abscess • Increases in CSF • hydrocephalus • Deficient CSF absorption or overproduction of CSF (Hogan & Hill, 2004)
Causes Cont’d • Increases in blood volume • epidural & subdural hematoma. • impaired blood flow to and from brain, • CO2, O2, • Hypertension
HYPERCAPNIA AND HYPOXIA • Any systemic process that affects blood levels of carbon dioxide will affect CBF, CPP and CBV because of cerebral vasodialation. • These conditions include respiratory inadequacy, poor ventilation, hyperventilation, drugs, and inadequate amounts of oxygen. Important!
Any process that results in increased ICP will produce impairment of content and arousal. Manifestations include any alteration in level of consciousness (restlessness, drowsiness, confusion) and a decrease in Glasgow Coma Scale (GCS) Clinical manifestations of increased ICP aresubtle!!!Diligent observation for changes in client’s condition. (Porth, C., 2004) Manifestations of Increasing Intracranial Pressure #1 RESTLESSNESS
Decreased level of consciousness Behavioral changes Headache Nausea & Vomiting Change in speech pattern Abnormal pupillary reactions Changes in body temperature Change in sensorimotor status Blurred or double vision (diplopia) Changes in cardiac rate & rhythm ataxia Seizures Cushing’s triad Abnormal posturing In addition may have:
CUSHING’S TRIAD! A response involving three classis signs: • widening pulse pressure: increased systolic BP with diastolic remaining the same or slightly elevated. • Bradycardia • Slowing respirations Cushing’s triad indicates increased severe ICP! Very Important!
Emergency Care • ABCs • Airway maintenance, intubation with oxygenation (PO2 > 90mmHg), mild hyperventilation – avoid hypercapnia. • Ensure adequate fluid however avoid lowering the blood osmolarity. • Initial neuro assessment and Glasgow Coma Scale • Etiology of the brain injury will dictate further evaluation & treatment
Emergency Care Cont’d • osmotic diuretics (mannitol IV) • steroids (controversial) • vasoactive medication (100-150mmHg systolic) • elevate HOB (30 degrees) • sedate as needed (barbituates IV) • drain CSF (keep ICP < 20) • maintain fluid status (normal serum Na & osmolality)