Download
1 / 53
530 likes | 673 Views
LIPIDS. An over view of Normal and Abnormal Lipids. All are One. This not about the GOD There is only one disease – Over nutrition Its faces are many such as Over weight / Obesity Diabetes mellitus, IR, Syndrome X Atherosclerosis – HT- CHD – CVD – RVD – PVD

E N D
LIPIDS An over view of Normal and Abnormal Lipids Downloaded from www.pharmacy123.blogfa.com
All are One • This not about the GOD • There is only one disease – Over nutrition • Its faces are many such as • Over weight / Obesity • Diabetes mellitus, IR, Syndrome X • Atherosclerosis – HT- CHD – CVD – RVD – PVD • Hyper lipidemias – endothelial dysfunction • Wear and tear of joints …. So on • What are we to do ? - Avoid over-indulgence Downloaded from www.pharmacy123.blogfa.com
How much is much ? BMI = Weight in kgs Height2 in mts 70 1.65 x 1.65 BMI = = 25.71 Underweight < 20 Over weight > 25 to 30 Normal 20 to 25 Obesity >30 Waist / Hip ratio = 35” /38” = 0.92 Normal for Males < 0.90, Females <0.80 Downloaded from www.pharmacy123.blogfa.com
Diets rich in Saturated Fat, Chol Sedentary Life Style Excess body weight/ Obesity Less perfect Genetic make-up Lipid abnormalities Atherosclerotic vascular disease CHD, CVD, PVD Lipid Abnormalities ROS tHcy Downloaded from www.pharmacy123.blogfa.com
Why are lipids important ? • Complications of Atherosclerosis are • CHD (Coronary Heart Disease) • CVD (Cerebro Vascular Disease) • RVD (Reno Vascular Disease) • PVD (Peripheral Vascular Disease) • These cause > 50% of all deaths - mortality • The Angina, MI, - TIA, Stroke, - HT, RF, - IC, Gangrene all reduce the Quality of Life - morbidity Downloaded from www.pharmacy123.blogfa.com
AVD – Clinical Manifestations For every thing the common denominator is ED Downloaded from www.pharmacy123.blogfa.com
Lipid Transport TG EC Apoprotein boat Apo A = HDL Apo B100+C+E = VLDL, IDL Apo B100 = LDL Apo B48+C+A+E = Chylomicrons Downloaded from www.pharmacy123.blogfa.com
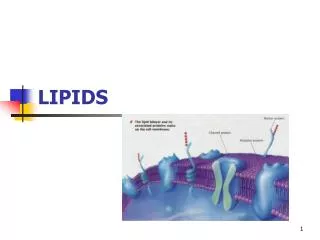
Lipids and Lipoproteins • Lipids or Fats in our body are mainly • The non polar, hydrophobic, inner core of • Triglycerides (TG) • Cholesterol Esters (EC) • The polar, surface monolayer • Phospholipids (PL) and Free Cholesterol (C) • Apoproteins are the outer coat -amphiphatic Downloaded from www.pharmacy123.blogfa.com
Lipoprotein Lipids or Fats (Hydrophobic) Size < RBC TG, EC Apoproteins A, B, C, E, (a) (Amphiphatic) Phospholipids Free Cholesterol (Hydrophilic) Downloaded from www.pharmacy123.blogfa.com
Lipoproteins Downloaded from www.pharmacy123.blogfa.com
Major Lipoproteins Downloaded from www.pharmacy123.blogfa.com
Lipoprotein Metabolism • Exogenous • Transport of dietary fats – TG to Adipose tissue, Muscle and Cholesterol to Liver as Chylomicrons • Endogenous • Transport of TG and CE from Liver to the peripheral tissues like muscle, adipose tissues and vascular endothelium via VLDL,IDL, LDL • Reverse Cholesterol transport –HDL Path • from the vessels and periphery to liver Downloaded from www.pharmacy123.blogfa.com
Enzymes • Lipo Protein Lipase (LPL) • Synthesized in Adipose and Muscle tissues • Essential for TG metabol – FFA and Glycerol • Insulin activates LPL,- CII apo binds to LPL • Hepatic TG Lipase (HGTL) • Removes TG from VLDL, IDL LDL • Clears the Cholesterol remnants into liver • Converts HDL2 to HDL3in the liver Downloaded from www.pharmacy123.blogfa.com
Enzymes contd.. • Lecithin Chol Acyl Transferase (LCAT) • Secreted into plasma by the liver • Binds to HDL and transfers linoleate from lecithin to free Chol and converts it into EC- • Cholesterol Ester Transfer Protein (CETP) • Secreted into plasma from liver • Transfers EC from HDL to VLDL • Converts LDL to small Dense LDL Downloaded from www.pharmacy123.blogfa.com
EXOGENOUS Downloaded from www.pharmacy123.blogfa.com
ENDOGENOUS Downloaded from www.pharmacy123.blogfa.com
HDLPATHWAY Downloaded from www.pharmacy123.blogfa.com
Lipid Peroxidation LDL, IDL Not normally taken up by the vessel wall ROS – Free radicals and Pro-oxidants Freely enters the vessel wall Oxidized LDL, IDL Macrophages Endothelium Scavenger pathway Foam Cells Cytokines, GF Atherosclerosis Downloaded from www.pharmacy123.blogfa.com
Synthesis of VLDL (TG) • In the liver VLDL is synthesized • It is dependent on substrate flow • Obesity • Excessive consumption of simple sugars • Increased intake of saturated fats • Inactivity • Alcoholism • Insulin resistance • Low HDL Downloaded from www.pharmacy123.blogfa.com
Primary Hyperlipidemia Downloaded from www.pharmacy123.blogfa.com
Secondary Hyperlipidemia Downloaded from www.pharmacy123.blogfa.com
Clinical Action • Presence of secondary causes of Hyperlipidemia • Order for full lipid profile (LP) – HT also • Presence of Hyperlipidemia – increased TG or EC • Investigate for all secondary causes • For all above 20 years once in every 5 years – LP • For those above 45 yrs – once in 2 years • For those with already known lipid abnormality follow-up every 3-6 months Downloaded from www.pharmacy123.blogfa.com
Lipid Profile Report Downloaded from www.pharmacy123.blogfa.com
LDLc Calculation LDLc = TC – (HDLc + TG/5) e.g. if TC = 250, HDLc = 50, TG = 150 LDLc = 250 – (50 + 150/5) = 250 – (50+30) = 250 – (80) LDLc = 170 Downloaded from www.pharmacy123.blogfa.com
Risk Factors for CHD Downloaded from www.pharmacy123.blogfa.com
Treatment Plan - LDLc Downloaded from www.pharmacy123.blogfa.com
Therapeutic Goals Downloaded from www.pharmacy123.blogfa.com
Cholesterol Levels Downloaded from www.pharmacy123.blogfa.com
Triglycerides NCEP Guidelines by expert panel on TG Downloaded from www.pharmacy123.blogfa.com
Diet Regimen Downloaded from www.pharmacy123.blogfa.com
Treatment Options • Diet – Two step approach • Drug therapy • HMG CoA Reductase Inhibitors • Bile Acid binding Resins • Nicotinic Acid • Fibric Acid derivatives • Probucol Downloaded from www.pharmacy123.blogfa.com
HMG CoA Red. Inh. • Called Statins – Atorvastatin, Simvastatin, Lovastatin etc., • 10 mg of Atorvastatin/Simvastatin OD, up to 40mg/day - • Synthesis of Cholesterol is blocked by inhibiting the enzyme hydroxy-methyl-Glutaryl Coenzyme A reductase • Increase in LDL receptors – traps LDL from plasma • Decrease in LDL by 25-45%, and VLDL TG by 10-20% • Increase HDL by 8-10%, No action on Lp(a) • Free of side effects - < 5%, Rise in Liver enzymes • Rare but serious complication is myopathy –CPK increase • Caution if combined with Gemfibrozil for combined hyperlipids. Downloaded from www.pharmacy123.blogfa.com
Nicotinic Acid • Decrease the synthesis of VLDL and LDL in liver • 50 – 100 mg t.i.d – increase up to 2 to 5g/day • Do not use sustained release preparation • Decreases TG by 25 to 85%, VLDL by 20-35% • Decreases LDL by 10-15%, may increase HDL? • Only agent – lowering Lp(a) by 25% • Flushing, pruritus, dry skin – tachycardia and atrial arrythmias – hyper uricemia, peptic ulcer disease, glucose intolerance, hepatic dysfunction • Poor side effect profile is the limitation. • Can be combined with resins, fibrates, statins Downloaded from www.pharmacy123.blogfa.com
Anion Resins • Interrupt the enterohepatic circulation of bile acids • Increased synthesis of bile acids–cholesterol sequestration • Cholestyramine (Questran) 378g containers or 4g sachets • Colestipol (Colestid) in 300g or 500g jars/5g packs/ 1g tab • Decrease LDL by 20-30%, Increase HDL and TG • Constipation, bloating, nausea, bleeding piles • Contra ind. : Biliary obstruction, G.Outlet obst., Incr. TG • Can be combined with Nicotinic acid, Statins Downloaded from www.pharmacy123.blogfa.com
Fibric Acid derivatives • Increase LPL activity – Increased hydrolysis of TG • Decrease VLDL synthesis, Increase LDL catabolism • Only Gemfibrozil is approved – 600mg b.i.d • Decrease TG by 25-40%, LDL may rise, modest rise HDL • Adv. Effects -Incr. Bile lithogenicity, abn. LFT, Myositis • Contr.In hepatic or biliary disease, caution in renal failure • Increase the anti-coagulant action of Warfarin • Can be combined with bile acid binding resins Downloaded from www.pharmacy123.blogfa.com
Probucol • Probucol (Lorelco) 500mg b.i.d with food • Third line drug – erratic effect on LDL & decrease of HDL • Lowers Cholesterol and only drug which regresses xanthomas • It is an antioxidant of LDL • Diarrohea, flatulence, nausea, increases QTc • Can be combined with bile acid sequestrating resins Downloaded from www.pharmacy123.blogfa.com
What is for what • If LDLc is more – Hypercholesterilimia alone • Statins 1st line – Simvastatin – Atorvastatin • Statins + Anion resin (Questron)– 2nd line • Or Statins + nicotinc acid – 2nd line • Probucol 3rd line specially for xanthomas • But not Statins + gemfibrozil • If TG alone is elevated – Hypertriglyceridemia • Gemfibrozil – 1st line • Nicotinic acid with or without Gemfibrozil– 2nd line • For mixed – combination- Statin+Nicotinic acid Downloaded from www.pharmacy123.blogfa.com
What’s in a name ? • Statins • Atorvastatin – Storvas, TG-tor, Avastin Simvastatin – Sim, Simvotin • Bile acid sequestering resins • Cholysteramine – Questron • Colistipal – Colestid • Nicotinic Acid – Niasyn • Fibric acid -Gemfibrozil– Lopid, Lipizyl • Probucol – Lorelco Downloaded from www.pharmacy123.blogfa.com
The Research Downloaded from www.pharmacy123.blogfa.com
The Future Research • We do not have yet any drug which increase the HDL • We do not know the precise role of Lp(a) and how to reduce it. • Small LDL needs further evaluation • RCTs to prove that the anti-oxidants have a real role to play both in treatment and in prevention of AVD Downloaded from www.pharmacy123.blogfa.com
Risk Factors for AVD • Hyperhomocyst(e)inemia • Diabetes mellitus • Hypertension • Dyslipidemia • Positive family history, Smoking, obesity and physical inactivity Oxidative Stress AVD Downloaded from www.pharmacy123.blogfa.com
Free Radical Formation Homolytic fission of a covalent bond Single covalent bond A B Homolytic fission Heterolytic fission B A A B Ions Free radicals Downloaded from www.pharmacy123.blogfa.com
ROS damage biological tissues- membranes Reactive Oxygen Species Lipid peroxidation Protein denaturation DNA Damage Free radicals released Cell Dysfunction and death Downloaded from www.pharmacy123.blogfa.com
Classification • Preventive antioxidants -Ceruloplasmin, transferrin, lactoferrin • Enzyme antioxidants -Superoxide dismutase, catalase, glutathione peroxidase • Scavenging or ‘chain-breaking’ or ‘sacrificial’antioxidants -Vitamins A,C, and E Downloaded from www.pharmacy123.blogfa.com
ROS and their Antioxidants Downloaded from www.pharmacy123.blogfa.com
Reactive Oxygen Species (ROS) ROS are highly reactive….and can damage biological tissues and membranes Downloaded from www.pharmacy123.blogfa.com
What is Homocysteine ? Metabolism Digestion Protein diet Methionine 1)Homocysteine Auto-oxidation Protein synthesis 2)Homocystine 3) Homocysteine thiolactone HS-CH2-CH2-CH-COOH Generation of ROS NH2 Homocysteine • 1+2+3= homocyst(e)ine • homocyst(e)ine = tHcy • Homocyst(e)inemia=hyper - tHcy • Sulfur-containing amino acid • By product of methionine metabolism Downloaded from www.pharmacy123.blogfa.com
Homocysteine : Metabolic Pathways Remethylation Cycle Demethylation Cycle Diet Tetra hydrofolate Methionine Folic acid MTHFR Vitamin B6 (MS) Methyl tetrahydrofolate Homocysteine Vitamin B6 (C beta S) MS – Methionine synthase MTHFR – Methyl tetrahydro folate reductase C beta S – Cystathionine beta synthase Cystathionine Transsulfuration Pathway Cysteine Sulphate Glutathione Downloaded from www.pharmacy123.blogfa.com
Hyperhomocyst(e)inemia Blood Homocyst(e)ine Levels • Moderate to severe hyper – tHcy : established risk factor for AVD 1-4 • Hyper – tHcy • - 5-7 % of the general population • - 12-47 % of patients with AVD Downloaded from www.pharmacy123.blogfa.com
Causes of Hyperhomocyst(e)inemia • Nutritional : Vitamin deficiency Folic Acid Vitamin B12 Vitamin B6 • Genetic : Enzyme Abnormality • Drugs : Methotrexate, Phenytoin, Theophylline Downloaded from www.pharmacy123.blogfa.com