Download
1 / 37
380 likes | 708 Views
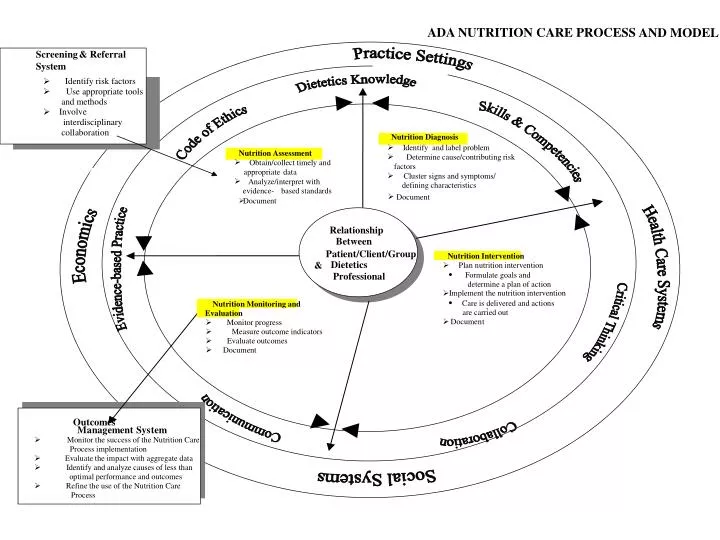
Ø. ADA NUTRITION CARE PROCESS. AND MODEL. Screening. & Referral. System. Ø. Identify risk factors. Ø. Use appropriate tools. and methods. Ø. Involve. interdisciplinary. collaboration. Nutrition Diagnosis. Ø. Identify and label problem. Nutrition Assessment. Ø.

E N D
Ø ADA NUTRITION CARE PROCESS AND MODEL Screening & Referral System Ø Identify risk factors Ø Use appropriate tools and methods Ø Involve interdisciplinary collaboration Nutrition Diagnosis Ø Identify and label problem Nutrition Assessment Ø Determine cause/contributing risk Ø Obtain/collect timely and factors appropriate data Ø Cluster signs and symptoms/ Ø Analyze/interpret with defining characteristics evidence - based standards Ø Document Document Relationship Between Patient/Client/Group Nutrition Intervention Dietetics & Ø Plan nutrition intervention · Professional Formulate goals and determine a plan of action Implement the nutrition intervention Ø · Care is delivered and actions Nutrition Monitoring and - are carried out Evaluation Ø Documen t Ø Monitor progress Ø Measure outcome indicators Ø Evaluate outcomes Ø Document Outcomes Management Sys tem Ø Monitor the success of the Nutrition Care Process implementation Ø Evaluate the impact with aggregate data Ø Identify and analyze causes of less than optimal performance and outcomes Ø Refine the use of the Nutrition Care Process
ADA’s Nutrition Care Process Steps • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
Nutrition Assessment (Definition) • “A systematic process of obtaining, verifying, and interpreting data in order to make decisions about the nature and cause of nutrition-related problems.” • Lacey and Pritchett, JADA 2003;103:1061-1072.
Nutrition Assessment Components • Gather data, considering • Dietary intake • Nutrition related consequences of health and disease condition • Psycho-social, functional, and behavioral factors • Knowledge, readiness, and potential for change • Compare to relevant standards • Identify possible problem areas
Nutrition Assessment: Critical Thinking • Observing verbal and non-verbal cues to guide interviewing methods • Determining appropriate data to collect • Selecting assessment tools and procedures and applying in valid and reliable ways • Distinguishing relevant from irrelevant data • Organizing data to relate to nutrition problems • Determining when problems require referral
ADA’s Nutrition Care Process Steps • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
Nutrition Diagnosis • Nutritional problem that the dietitian is responsible for treating • Names and describes the problem • Problem may already exist, or may be at risk of occurring • Not a medical diagnosis • Type 2 diabetes = medical diagnosis • Excessive carbohydrate intake resulting in elevated blood glucose levels = nutrition diagnosis.
Nutrition Dx Domains: Intake Defined as “actual problems related to intake of energy, nutrients, fluids, bioactive substances through oral diet or nutrition support (enteral or parenteral nutrition) • Class: Calorie energy balance • Class: Oral or nutrition support intake • Class: Fluid intake balance • Class: Bioactive substances balance • Class: Nutrient balance
Nutrition Dx Domains: Clinical Defined as “nutritional findings/problems identified that relate to medical or physical conditions • Class: functional balance (change in physical or mechanical functioning with nutritional consequences) • Class: Biochemical balance: change in capacity to metabolize nutrients as a result of medications, surgery, or as indicated by altered lab values • Class: weight balance: chronic weight or changed weight status when compared with usual or desired body weight
Nutrition Dx Domains: Behavioral-Environmental Defined as “nutritional findings/problems identified that relate to knowledge, attitudes/beliefs, physical encironment, or access to food and food safety • Class: knowledge and beliefs • Class: physical activity, balance and function • Class: food safety and access
Nutrition Diagnosis Components • Problem (Diagnostic Label) • Etiology (Cause/contributing risk factors) • Signs/Symptoms (Defining characteristics) • Signs = objective data = observable, measurable changes • Symptoms = subjective data = changes pt feels and expresses
Nutrition Diagnosis Components • Problem (Diagnostic Label) • Describes alterations in pt’s nutritional status • Diagnostic labels • Impaired (nutrient utilization…) • Altered (GI function…) • Inadequate/excessive (calorie intake…) • Inappropriate (intake of types of carbohydrate) • Swallowing difficulty
Nutrition Diagnosis Components • Etiology (Cause/Contributing Factors) • Related factors that contribute to problem • Identifies cause of the problem • Helps determine whether nutrition intervention will improve problem • Linked to problem by words “related to” (RT) • Note: etiology may not always be clear
Nutrition Diagnosis Components • Etiology (Cause/Contributing Factors) • Excessive calorie intake (problem) related to regular consumption of large portions of high-fat meals (etiology) • Swallowing difficulty (problem) related to stroke (etiology)
Nutrition Diagnosis Components • Signs/Symptoms (Defining characteristics) • Evidence that problem exists • Linked to etiology by words “as evidenced by”
Nutrition Diagnosis Components • Etiology (Cause/Contributing Factors) • Excessive calorie intake (problem) “related to” regular consumption of large portions of high-fat meals (etiology) as evidenced by diet history and weight status • Swallowing difficulty (problem) related to stroke (etiology) as evidenced by coughing following drinking of thin liquids (signs and symptoms)
Nutrition Diagnosis • Excessive calorie intake (P) • “related to” regular consumption of large portions of high-fat meals (E) • “as evidenced by” diet history & 12 lb wt gain over last 18 mo (S & S)
Nutrition Diagnosis Components • Food, nutrition and nutrition-related knowledge deficit (P) R/T lack of education on infant feeding practices (E) as evidenced by infant receiving bedtime juice in a bottle (S) • Altered GI function (P) R/T ileal resection (E) as evidenced by medical history and dumping syndrome symptoms after meals (S)
Nutrition Diagnosis Components Nutrition Diagnosis Statement should be: • clear, concise • specific • related to one problem • accurate – related to one etiology • based on reliable, accurate assessment data
ADA’s Nutrition Care Process Steps • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
Nutrition Intervention Definition • “Purposely-planned actions designed with the intent of changing a nutrition-related behavior, risk factor, environmental condition, or aspect of health status for an individual, a target group, or population at large.” – • Lacey and Pritchett, JADA 2003;103:1061-1072 • Directed at the etiology or effects of a diagnosis
Intervention Objectives Should be patient-centered • Must be achievable • Stated in behavioral terms, quantifiable terms • Pt and counselor must establish goals together • may involve other members of health care team • What will the patient do or achieve if objectives met
Intervention Objectives • Problem 1: Involuntary weight loss • Objectives: • 1. Pt will stop losing wt and begin to gain wt slowly, to a target wt of 145# • 2. Pt will modify his diet to increase intake to meet calorie and protein needs
Intervention Objectives • Problem 2: Inadequate protein-energy intake 2° poor appetite • Objectives: • 1. Pt will attend senior center for lunch daily to improve socialization and calorie intake • 2. Pt will include nutrient-dense foods in his diet
Nutrition Intervention • Intervention translates assessment data into strategies, activities, or interventions that will enable the patient or client to meet the established objectives. • Interventions should be specific: —What? —When? —Where? —How?
Nutrition Intervention • Problem 1: Involuntary Weight loss • Intervention: • Pt will try to eat three meals a day plus bedtime snack • Pt will include at least one nutrient-dense supplement per day in his diet • Pt will increase energy intake to 1800 kcal per day, complete 3-day food record for analysis of adequacy
Nutrition Intervention • Problem 2: Inadequate protein-calorie intake 2° poor appetite • Intervention: • Pt will include nutrient-dense foods with meals, especially when appetite is minimal • Patient will begin meal with nutrient-dense foods, follow with others • Pt will attend senior center for lunch daily to improve socialization/appetite
ADA’s Nutrition Care Process Steps • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
Nutrition Monitoring & EvaluationComponents Evaluate outcomes Compare current findings with previous status, intervention goals, and/or reference standards
What gets Measured? Nutrition Monitoring and Evaluation Types of Outcomes • Direct nutrition outcomes • Clinical and health status outcomes • Patient/client-centered outcomes • Healthcare utilization Intermediate-result outcome End-result outcome
Nutrition Goals and Objectives • Are necessary in order to evaluate the effectiveness of nutrition care • Should be achievable and based on scientific evidence • Should be directly or indirectly related to nutrition care
NCP Example: Acute Care Nutrition Assessment • Medical hx: 72 y.o. female admitted with decompensated CHF; heart failure team consulted; has been admitted with same dx x 2 in past month; meds: Lasix and Toprol; current diet order: 2 gram sodium; has lost 5 pounds in 24 hours since admission; Output > input by 2 liters • Nutrition history: has been told to weigh self daily but has no scale at home. Does not add salt to foods at the table. Noticed swollen face and extremities on day prior to admission. Day before admission ate canned soup for lunch and 3 slices of pizza for dinner; does not restrict fluids; has never received nutrition counseling
NCP Example: Acute Care Nutrition Diagnosis • Excessive sodium intake r/t frequent use of canned soups and restaurant foods as evidenced by diet history • Knowledge deficit r/t no previous nutrition education as evidenced by frequent use of high sodium convenience foods and inability to name high sodium foods • Excess fluid intake r/t dietary indiscretions as evidenced by diet hx and current fluid status • Self-monitoring deficit r/t lack of access to scale as evidenced by patient self report
NCP Example: Acute Care Nutrition Intervention • Excessive sodium intake: Patient will attend Senior Feeding site that provides low sodium meals; Patient will implement survival skills low sodium diet principles and attend heart failure diet program in heart failure clinic • Self-monitoring deficit: Patient will obtain free home scale from CHF case manager; will limit fluids to 2 liters/day per instructions in Heart Failure Clinic if adherence to low sodium diet does not achieve appropriate fluid balance
NCP Example: Acute Care Monitoring and Evaluation • Patient will weigh self daily and keep log; report to heart failure case manager if weight ↑ 2 lb in 24 hours • Patient will bring 3 day diet record to heart failure clinic for review by dietitian • Heart failure case manager will track hospital readmissions over 12 months