Download
1 / 41
460 likes | 1.09k Views
Acute Pericarditis and Pericardial Effusion. Meghan York September 9, 2009. Outline. Anatomy of pericardium Overview of pericardial disease Etiology Clinical presentation Ancillary diagnostics 6) Echocardiography in evaluation. Anatomy. Normal amount of pericardial fluid: 15-50 cc

E N D
Acute Pericarditis and Pericardial Effusion Meghan York September 9, 2009
Outline • Anatomy of pericardium • Overview of pericardial disease • Etiology • Clinical presentation • Ancillary diagnostics 6) Echocardiography in evaluation
Anatomy • Normal amount of pericardial fluid: 15-50 cc • Two layers: • Outer layer is the parietal pericardium and consists of layers of fibrous and serous tissue • Inner layer is visceral pericardium and consists of serous tissue only
Pericardium • Fibroelastic sac consisting of 2 layers • Visceral at epicardial side • Parietal at mediastinal side • Pericardial fluid formed from ultrafiltrate of plasma
Diseases of the Pericardium • Acute Fibrinous Pericarditis • Pericardial Effusion • Cardiac tamponade • Recurrent Pericarditis • Constrictive Pericarditis
Epidemiology of Acute Pericarditis • 0.1% of hospitalized patients • 5% of patients admitted to Emergency Department for non-acute myocardial infarction chest pain
Findings on Echo • Pericardial effusion • If present, possibility of tamponade physiology needs to be considered • Pericardial thickening • Increased echogenicity of pericardial reflection and as multiple parallel reflections posterior to the LV on M-mode • If present, evidence of constrictive physiology should be considered
Chest X ray • Normal in patients with acute pericarditis unless pericardial effusion is present • Enlarged cardiac silhouette • Requires 200cc of fluid
Major Causes of Pericardial Disease 1)Infection 2)Radiation 3)Neoplasm 4)Myocardial intrinisic disease 5)Trauma 6)Autoimmune 7)Drugs 8)Metabolic *viral, autoreactive/autoimmune, and neoplastic most common diagnosis
Viral -adenovirus -enterovirus -cytomegalovirus -influenza -hepatitis B -herpes simplex -echovirus -mumps Mycoplasma Fungal Parasitic Bacterial -staphylococcus -streptococcus -pneumococcus -haemophilus -neisseria -chlamydia -legionella -tuberculous -lyme disease Etiology of Acute Pericarditis: Infectious
Radiation Neoplasm -metastatic -primary cardiac -paraneoplastic Cardiac -early infarction -Dressler’s -myocarditis -aortic dissection Trauma -blunt -iatrogenic (perforations, post-surg) Autoimmune -rheumatic disease -non-rheumatic -Wegners, sarcoid, IBD Etiology: continued
Drugs -drug induced lupus hydralazine isoniazid procainamide -doxorubicin -phenytoin Metabolic -hypothyroid -uremia -ovarian hyperstimulation Etiology: continued
Lab Testing • the historic yield of diagnostic evaluation is low, typically only in 16% of patients is etiology determined. • evaluation of pericardial fluid and tissue with tumor markers, PCR, immunohistochemistry, flourescence-activated cell sorting has shown a trend toward higher yield of diagnosis
Diagnosis of Pericarditis: Presence of two of the following necessary 1) Chest pain • Sudden onset • localized to anterior chest wall • pleuritic • sharp • Positional: may improve if pt leans forward, worse with lying flat 2) Cardiac auscultation: Pericardial friction rub • Present in up to 85% of pts with pericarditis without effusion • friction of the two inflamed layers of pericardium, typically triphasic rub, heard with diaphragm of stethoscope at left sternal border 3) Characteristic ECG changes 4) Pericardial effusion
Pertinent Lab Results • Elevated C reactive protein level • strong correlation - normal CRP makes acute pericarditis diagnosis less likely • Elevated CK, CK-MB, and Troponin • Often elevated Troponin alone • Indicates inflammation of myocardium just beneath the visceral pericardium • Not associated with worse outcomes • Leukocytosis
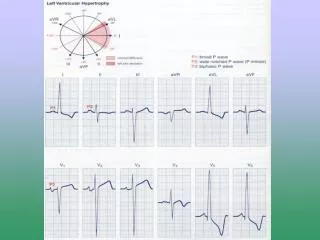
ECG Findings: 60% of patients • Stage 1: hours to days • Diffuse ST elevation -sensitive v5-v6, I, II • ST depression I/aVR • PR elevation aVR • PR depression diffuse -especially v5-v6 • PR change is marker of atrial injury • Stage 2: • Normalization
Stage 3: Diffuse T wave inversions ST segments isoelectric Stage 4: EKG may normalize T wave inversions may persist indefinitely ECG changes over weeks
STEMI or Pericarditis by ECG • ST elevation in pericarditis • Starts at J point • Rarely exceeds 5mm • Retains normal concavity • Non-localizing • Arrhythmias very unlikely in pericarditis (suggest myocarditis or MI)
Acute Pericarditis • 51yo man with acute onset sharp substernal chest pain two days prior
Pericardial Effusion • Low voltage and Electric Alternans
ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: summary article • Recommended specific circumstances for use of echocardiography in pericardial disease
Class I Recommendations 1. Patients with suspected pericardial disease, including effusion, constriction, or effusive-constrictive process. 2. Patients with suspected bleeding into the pericardial space (trauma, perforation, dissection)
Class I (continued) 3. Follow-up study to evaluate recurrence of effusion or to diagnose early constriction; repeat studies may be goal directed to answer a specific clinical question 4. Pericardial friction rub developing in acute myocardial infarction accompanied by symptoms such as persistent pain, hypotension, and nausea.
Class IIa 1)Follow-up studies to detect early signs of tamponade in the presence of large or rapidly accumulating effusions. A goal-directed study may be appropriate. 2)Echocardiographic guidance and monitoring of pericardiocentesis.
Class IIb 1) Postsurgical pericardial disease, including postpericardiotomy syndrome, with potential for hemodynamic impairment. 2) In the presence of a strong clinical suspicion and nondiagnostic TTE, TEE assessment of pericardial thickness to support a diagnosis of constrictive pericarditis.
Pericardial Fat Pad • Often pericardial fat pads can be seen in this view anterior to the RVOT • Fat pads usually not seen elsewhere
Posterior Effusions • Pericardial effusions can track posteriorly toward sinus • In this case, may only be seen in axial 4 chamber view
Tamponade • Pressure in pericardium exceeds pressure in the cardiac chambers, lower chamber atria affected before higher pressure ventricles • Compressive effect is seen best in the phase when the intrachamber pressure is lowest – systole for atria and diastole for ventricles • Diagnostic techniques • 2D looking for RA/RV collapse during diastole • M-mode for RA/RV collapse during diastole • Doppler of Mitral and Tricuspid inflow • Mitral inflow to decrease by 25% with inspiration • Tricuspid inflow increased by 40% with inspiration • IVC diameter fails to increase with inspiration