Download
1 / 103
1.04k likes | 1.43k Views
Sepsis Syndromes. Aric Storck October 5, 2006. Objectives. Review of basic pathophysiology Overview of treatment with focus on ED care Initial resuscitation Infection & source control Early goal directed therapy Ventilatory strategies Pharmacologic therapies. Epidemiology.

E N D
Sepsis Syndromes Aric Storck October 5, 2006
Objectives • Review of basic pathophysiology • Overview of treatment with focus on ED care • Initial resuscitation • Infection & source control • Early goal directed therapy • Ventilatory strategies • Pharmacologic therapies
Epidemiology • Most common non-cardiac cause of death in ICU • Disproportionately affects elderly, HIV, chemotherapy, transplant, dialysis, diabetes, alcoholics • Accounts for 215,000 deaths/yr in US = MI deaths or 9.3% of all deaths in 1995 • Annual cost in US $16.7 billion • Locally ~250 ICU admissions for sepsis per year
Systemic Inflammatory Response Syndrome • “a systemic inflammatory response to a variety of clinical insults.” • Diagnostic Criteria = 2 or more of • T >38 or <36 • HR > 90 • RR > 20 or PCO2 < 32 • WBC > 12 or < 4 or >10% bands • Problems • Too simplistic & extremely non-specific
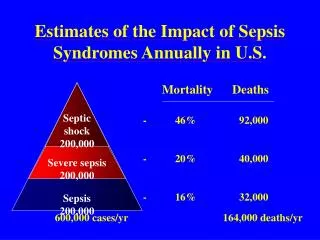
SIRS & Sepsis • Infection • invasion of organ system(s) by microorganisms • Sepsis • SIRS + infection • Severe sepsis • Sepsis with organ dysfunction • Lactic acidosis, oliguria, ALOC, etc. • Responsive to fluids • Septic shock • Severe sepsis requiring vasopressors/inotropes to maintain normotension
Sepsis Spectrum & Mortality Diagnostic categoryMortality (%) SIRS criteria none 3 2 7 3 10 4 17 Sepsis 16 Severe sepsis 20 Septic shock 46 McCoy & Matthews. Drotrecogin Alfa (Recombinant Human Activated Protein C) for the treatment of severe sepsis. Clin Ther 2003; 25: 396-421
Sepsis Etiology • > 90% bacterial • Gram negative ~42% • Gram positive ~34% • Anaerobes ~2-5% • Mixed ~14% • Fungi ~5% • Primarily Candida • More common in ICU, immunocompromise, steroids, diabetics Llewelyn & Cohen. Diagnosis of infection in sepsis. Int Care Med. 2001; 27: S10-32 Bochd, Glauser, & Calandra. Antibiotics in sepsis. Int Care Med. 2001; 27: S33-48
Sources of Infection • Specific sites: • Respiratory 36% • Blood 20% • Abdomen 19% • Urinary tract 13% • Wounds & Skin 7% • Other 5% • Can be identified in ~92% of pts • Extremely important in choosing Abx Bochd, Glauser, & Calandra. Antibiotics in sepsis. Int Care Med. 2001; 27: S33-48
Not all that is febrile & shocky is infectious… • Non-infectious causes of SIRS • Tissue damage • Surgery, trauma, DVT, MI, PE, pancreatitis, etc • Metabolic • Thyroid storm, adrenal insufficiency • Malignancy • Tumor lysis syndrome, lymphoma • CNS • SAH • Iatrogenic • Transfusion rx, anesthetics, NMS, etc Llewelyn & Cohen. Diagnosis of infection in sepsis. Int Care Med. 2001; 27: S10-32
International consensus guidelines • Provide guidance on • Initial resuscitation • Source control • Drugs • Fluid therapy • Blood products • Mechanical ventilation
Treatment of Septic Shock Antibiotics Surgical Management EGDT Steroids Ventilation rhAPC
Case 1 • 76 F – from nursing home • Increasing confusion x 3 days • Not eating • Complaining of lower abdominal tenderness • O/E • HR 105 RR 30 BP 95/62 Sats 91% T 38.1 • CVS – Normal HS • Chest – Decreased A/E to bases, no distress • Abdo - soft, +BS, Moderate periumbilical and suprapubic tenderness
Case 1 - Investigations • ECG – sinus tach • CXR – cardiomegaly, hyperinflation, nil acute • Lab • CBC • Hb 94; WBC 11 (bands 2); platelets 154 • Lytes • Na 133 K 4.9 Cl 98 HCO3 18 • LFT’s – normal • Urine - +nitrites, + leuks, >30 WBC
Case 1 - continued • Diagnosis? • Does this patient have SIRS? • Sepsis? • Severe Sepsis? • Septic Shock? • Initial Management?
Which fluid are you going to give? Fluid Resuscitation
DBRCT, N=6997. • 4% albumin vs crystalloid • Amount titrated to clinical status and response to fluids • Primary outcome: 28d mortality • 18% patients had severe sepsis
Crystalloid vs Colloid • Cochrane Systematic Reviews, 2005. • Albumin or plasma protein fraction. • 19 Trials reported data on mortality • N= 7576 • RR from these trials was 1.02 (0.93, 1.11). • No evidence of meaningful benefit to colloids vs crystalloids • Normal Saline • Cheap, available • USE IT FIRST • How much are you going to give?
EGDT – Fluid Resuscitation • EGDT • Step 1 – Fill the tank • Normal Saline • 500ml bolus then 500ml q30min until CVP 8-12 • How can you measure CVP in the ED? • What if the patient is intubated • Target a CVP 12-15 to account for increased intrathoracic pressure
Surviving Sepsis Guidelines - Fluids • No evidence for choosing colloid over crystalloids (Grade C) • Administer crystalloids as 500-1000 cc over 30 mins & repeat prn based on response (E) • Administer colloids at 300-500 cc over 30 mins & repeat prn based on response (E)
Surviving Sepsis Guidelines - Fluids • “resuscitation…should not be delayed pending ICU admission.” • Goals of resuscitation in 1st 6 hrs of recognition: (B) • CVP: 8-12 mm Hg (12-15 if ventilated) • MAP: > 65 mm Hg • Urine output: > 0.5 ml/kg/hr • SVO2 > 70% • If unable to attain SVO2 >70% despite above then: • Transfuse to keep Hct > 30% • Dobutamine Dellinger et al. Surviving sepsis campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004; 32: 858-73
Back to Case 1 • After 2500ml of NS CVP is ~10 • You reassess the patient • O/E • HR 100 RR 32 BP 80/50 Sats 91% T 38.4 • What is their MAP? • What is your next move?
Vasopressors • Goals • MAP >65 • Improvement in indicators of end organ perfusion • Which vasopressor do you choose? • What is your starting dose?
Dopamine Precursor of epi/norepi Release of norepi from presynaptic terminals Dosing Dopaminergic <5ug/kg/min Vasodilation coronary, renal, mesenteric beds Beta - 5-10ug/kg/min Increase contractility and HR Alpha - >10ug/kg/min vasoconstriction Norepinephrine Alpha agonist Increases BP by vasoconstriction, little effect on HR or cardiac output Dosing Start at 0.1 ug/kg/min Double every five minutes to effect Maximum ~ 2ug/kg/min Vasopressors
Dopamine vs Norepinephrine • Theoretical advantages to norepinephrine • Direct acting, works in catecholamine depleted patients • Less tachycardias & dysrhythmias • Indirect evidence of benefit over dopamine in multiple small trials • Improved hemodynamics • Improved gastric pH • Improved lactate • Single non-randomized trial showing mortality benefit • No RCT showing mortality benefit
Surviving Sepsis Guidelines - Vasopressors • Should be used when • shock refractory to fluid resuscitation • Life-threatening hypotension (E) • Dopamine or norepinephrine are 1st line agents (D) • ‘Renal dose’ dopamine does not work & should not be used (B) • Invasive BP monitoring & central IV lines should be placed as soon as possible (E) • Vasopressin may be considered as a 2nd line agent in refractory shock (E)
Back to our case • Our patient now on dopamine 10ug/kg/min • VS 120 RR 30 BP 95/65 Sats 92% T 38.1 • You now have a few moments to think • You’re pretty sure this patient has Urosepsis? • What else would you like to do?
Antibiotics & Source Control “Autopsy studies in persons who died in the intensive care unit show that failure to diagnose and appropriately treat infections with antibiotics or surgical drainage is the most common avoidable error” Hotchkiss & Karl. The pathophysiology and treatment of sepsis. N Eng J Med. 2003; 348: 138-50
Do Antibiotics make a difference? • Animal models • increased mortality with each hour of delay to antibiotics • Few prospective RCT’s • most outcome data based on retrospective analyses • ARR 16 – 26% when initial Abx were appropriate • Virtually all studies in ICU setting • Prospective cohort study of 406 pts w/ sepsis found inadequate initial Abx Tx significantly increased risk of death in non-surgical sepsis (OR 8.15; 95%CI 1.98-33.5) • Adequate Tx dec’d risk of death in surgical sepsis (OR 0.37, 95%CI 0.18-0.77) Garnacho-Montero et al. Impact of adequate empirical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis. Crit Care Med 2003; 31: 2742-51
Community Acquired Pneumonia Ceftriaxone 2gm IV PLUS Azithromycin 500mg IV OR Levofloxacin 500mg IV Intra-abdominal Infection Piperacillin/Tazobactam 3.375gm IV OR Ceftriaxone 2gm IV PLUS Flagyl 500mg IV OR Ampicillin 2gm IV PLUS Gentamicin 6mg/kg IV PLUS Metronidazole 500mg IV Urosepsis Gentamicin 6mg/kg IV OR Ceftriaxone 2gm IV Meningitis Dexamethasone 10 mg IV at or before antibiotics given Ceftriaxone 2 gm IV PLUS Vancomycin 1 gm IV Cellulitis/Bone/Joint Cefazolin 2 gm IV OR Cloxacillin 1 gm IV Fasciitis Clindamycin 600 mg IV PLUS Penicillin 4 MU IV PLUS IVIG PLUS Surgery Endocarditis Ensure Blood Culture x THREE are done Ceftriaxone 2gm IV ADD Vancomycin 1 gm IV if MRSA suspected Infected Central Line Pull Line Vancomycin 1 gm IV Neutropaenic Piperacillin/Tazobactam 3.375gm IV PLUS Gentamycin 6 mg/kg IV Sepsis Source Unknown Treat for MOST likely source Treat as per Intra-abdominal Infection CHR Sepsis Protocol Recommendations
Blood cultures • Important to establish Dx for: • Guiding antimicrobial Tx • Guiding adjunctive Tx • Microbiological epidemiological surveillance • Llewelyn & Cohen. Diagnosis of infection in sepsis. Int Care Med. 2001; 27: S10-32 • Yield of cultures ranges from 9-64% • Bochd, Glauser, & Calandra. Antibiotics in sepsis. Int Care Med. 2001; 27: S33-48 • Don’t forget to draw cultures before antibiotics!
Blood cultures • Limitations • Colonization vs. infection • Prior antimicrobial Tx • Significance of • Rare or unfamiliar organisms • Mixed culture results • Organisms not usually associated with disease Llewelyn & Cohen. Diagnosis of infection in sepsis. Int Care Med. 2001; 27: S10-32
Surviving Sepsis Guidelines-Antibiotics • Draw appropriate cultures first • Give antibiotics within 1 hr of recognition of septic syndrome • Antibiotics should be broad-spectrum & chosen to cover most likely organisms based on presentation & local resistance patterns • Arrange for further diagnostic studies to rule out surgically correctable foci of infection once appropriate
Surviving Sepsis Guidelines - Source Control • Get appropriate study to find the source (CT, U/S, etc.) • Choose least invasive effective intervention • eg. CT guided percutaneous drainage vs surgery • Source control ASAP after initial resuscitation • Remove any possible iatrogenic sources • Central lines, foley catheters, etc.
Back to our case • You started our patient on gentamicin • He’s still on dopamine 10ug/kg/min • VS 120 RR 30 BP 95/65 Sats 92% T 38.1 • What would you like to do now?
Measurement of ScvO2 • What is ScvO2? • Reflects oxygenation at tissue level • How are you going to measure ScvO2? • What is the difference between mixed venous and central venous SvO2? • ScvO2 • blood from SVC or right atrium • SmvO2 • blood from pulmonary artery • Contains blood from IVC (lower extremity) and coronary sinus • ScvO2 and SmvO2 correlate well
ScvO2 • What is a normal ScvO2 • Normal ~75% • Normal pO2 ~40 • ScvO2 comes back • ScvO2 = 64% • What does this result mean?
Repeat CBC • Hb 81 Hct 0.25 • What do you do • Transfuse patient to Hct of 0.3 • What is the physiological rationale for transfusion • O2 content = (1.34 x Hb x SaO2) + (0.0031 x PO2)
Transfusion in Sepsis • 95% of ICU pts anemic by day 3 of ICU stay • Mechanisms • Phlebotomy = average 65 ml/day • Ongoing bleeding • Fluid resuscitation • Underproduction anemia • Blunted erythropoietin response secondary to inflammatory cytokine production • Abnormal iron metabolism due to immune activation • Low iron levels & elevated ferritin Corwin et al. Transfusion practice in the critically ill. Crit Care Med 2003; 31(S): S668-71
When should you transfuse? • Surviving Sepsis Guidelines • Transfuse to keep Hb > 70 g/L unless extenuating circumstances (e.g. CAD) (B) • Based on TRICC trial • Rivers et al. 2001 • Transfuse to keep hematocrit at least 30%
Multicenter RCT of 838 ICU pts w/ Hb <90 • Randomized to • Liberal strategy • Transfusion threshold 100 g/L – aim for 100 -120g/L • Restrictive strategy (study group) • Transfusion threshold 70 g/L – aim for 70 – 90 g/L • Primary outcome • All cause mortality at 30 days
TRICC Trial • Results • No difference in 30 or 60 day mortality • Lower in-hospital mortality in restrictive group • 22.2% vs 28.1% (p=0.005) • No difference in mortality in sepsis sub-group • But only 5% of patients had sepsis • Less sick pts (APACHE II score <20) did better with restrictive strategy • ARR 7.4% (95%CI 1.0 – 13.6%) • Conclusion • Restrictive strategy equivalent to, and possibly better than keeping Hb > 100 g/L
Reconciling EGDT and TRICC • EGDT • Hypovolemic patients • Actual measurement of suboptimal O2 delivery • Early resuscitation phase • TRICC • Euvolemic pts enrolled within 72 hours of ICU • Only 6% sepsis, only 27% had any infection • Bottom Line • Use EGDT in acute resuscitation, use TRICC afterwards when stabilized
Surviving Sepsis Guidelines - Transfusion • “Once tissue hypoperfusion has resolved and in the absence of extenuating circumstances, such as significant coronary artery disease, acute hemorrhage, or lactic acidosis (see recommendations for initial resuscitation), red blood cell transfusion should occur only when hemoglobin decreases to 70 to a target Hb of 70-90.” • Recommends EGDT in initial resuscitation