Download
1 / 36
370 likes | 710 Views
Diagnosis Of A Case Of Anemia. Prof Sameh Shamaa Prof Of medical Oncology and Internal medicine Mansoura Faculty Of Medicine. Anemia. Def : Reduction in the concentration Of HB in the peripheral blood below the normal for the age and sex of the patient: <13 gm. /100 ml for adult male

E N D
Diagnosis Of A Case Of Anemia Prof\ Sameh Shamaa Prof Of medical Oncology and Internal medicine Mansoura Faculty Of Medicine
Anemia Def : Reduction in the concentration Of HB in the peripheral blood below the normal for the age and sex of the patient: • <13 gm. /100 ml for adult male • <11.5 gm./100 ml for adult female & infant • <14 gm. /100 ml for new born
False Anemia HB concentration Normal ↓ True Anemia ↓ False Anemia 1- Preg. 2nd trimester 2- Large spleen3- ↑ immunoglobulin
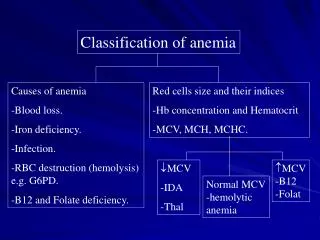
Classification Depends on: I- Aetiology. 2- morphology of RBCs both are complementary
I- Anemia due to excess red cell loss: a) Post- haemorrhagic anemia - Acute haemorrhagic Anemia - Chronic Haemorrhagic Anemia b) Haemolytic anemia - corpuscular defect - Extra corpuscular defect
II- Anemia due to impaired red cell formation • disturbance of B.Mfunction due to deficiency of substances essential for erythropoiesis: - Substance essential for HB synthesis: - Iron deficiency anemia - Protein deficiency - Substance necessary for DNA synthesis : - Folic acid - B12
disturbance of B.M. function Not due to deficiency. of substances essential for erythopoiesis • due to B.M. infiltration • Aplastic Anemia
III- Anemia due to other causes : 1- endocrine disorders 2- renal failure 3- Infections 4- liver disease 5- malignant disease 6- collagen diseases
Clinical Picture The symptoms and signs are due to: I: The anemia itself. II: The disorder causing the anemia.
I- Clinical picture of Anemia Whatever the cause: • Symptoms: • Generalized • C.V.S • CNS b) Signs : • Pallor • C.V.S : Tachycardia High C.O. state Murmurs Congestive heart Failure
II- Clinical picture which may indicate the cause of anemia:- • History:
a) Present History : • Age and sex • Occupation • Rate of onset • History or blood loss • History or bleeding tendency
History suggestive of hemolysis • History of drug intake - G.I.T symptoms - Bony pains - C.N.S paraesethia - Fever • Diet b) Social History c) Menstrual and Gynecologic History d) Family History
General examination: • Built • Skin • purpura, ecchymosis • Conjunctiva • Mouth • Nails • Blood pressure • Bones • Legs
B) C.V. examination : - Hypertension - Signs are usually secondary to anemia. - Presence of organic heart disease may suggest rheumatic activity or bacterial endocarditis C) Abdominal examination : • Splenomegaly • Hepatomegaly - Abdominal mass
I- Determination of the morphologic type : - Microcytic and or hypochromic . - Normochromic (Normocytic or microcytic). - Macrocytic (Megaloblastic or Normoblastic ). According to : • MCV • MCHC • Reticulocytic count
II- Discovery of the cause : From:- - history. - physical examination. - blood film examination. - Sometimes+ further special investigation.
A-Microcytic +/- hypochromic. M.C. HC ≤ 32% and/or M.C.V ≤80N2 ↓serum iron serum iron ↑ (≤60 ug ♀or ≤ 70 ug ♂) (≥60 ♀, ≥ 70 ♂ ug%) ↓ TIBC Abn.Hb Sideroblastic with ↑Retculocytes (congenital) ↑TIBC ↓ TIBC Iron deficiency inflammatory Hb electrophoresis Iron stain of BM (Thalassemia)
If iron deficiency anemia: Search for a source of chronic blood loss: 1)In females: -Abnormal uterine bleeding;menorrhagia or contra- ceptive device. -Gynaecologic examination for fibroids or tumours. 2)G.I.bleeding: -Occult blood ,parasites. -Barium meal or upper endoscopy. -Colonoscopy or barium enema. 3)Less frequent causes:*Iron deficiency;malabsorption. *Chronic epistaxis or hematuria.
B-Normochromic Anemia with Reticulocytosis Reticulocytes >120. 000/mm3 M.C.V. N. or slightly ↑ Anemia with regeneration.
1) signs of acute heamorrhage - epistaxis - h.± melena - hemoptysis Post hemorrhagic Anemia Normochromic Anemia with Reticulocytosis
Normochromic Anemia with Reticulocytosis 2) If No evidence of He but signs of hemolysis and/or : ↑ indirect bilirubin ↓ Haptoglobine Hemolytic Anemia Search for the most commonacute causes: *Coomb’s test *G6PD *Blood culture (septicemia)*Malaria
Normochromic Anemia with Reticulocytosis If (1),(2) are negative - repair of certain anemias e.g tretment with B12 or folic - stopage of toxins fore erythropoises. e.g alcohol, chloramphenicol. - Rcent unnoticed Hemorrhage.
Normochromic Anemia with Reticulocytosis Search for abnormalities Of RBCs in blood film Microspherocytosis other abnormalities in shape or size family history and Hb electrophoresis osmotic fiagility test
Normochromic Anemia with Reticulocytosis if No abnormalities In R.B.C family history associated chronic presence of urinary disease pigmentation search for abn. if Hb - Hb - Enzyme cirrhosis, S.L.E PNH - Membrane lymphatic leuk. Lymphoma. Ham’s test repeat coomb,s
C-Aregenerative Non Microcytic Anemia: i.e., Normochromic , Normocytic or macrocytic Anemias (MCV > 82 N2 , MCHC > 32% , reticulocytes < 120.000 ) If Hb < 8 gm., ret. Must be > 100.000 if ↓ ---- Aregenerative anemia But anenria must be > 1 week duration Insufficient production by the marrow History (alcoholism, drug's …); WBCs and, platelets (i.e., do blood film) (1) Alcoholism mod. (2) Normocytic anemia (3) No alcohol (4) Neutropenia Macrocytosis<110 Normal WBCs & + macrocytosis + Platelets Bone marrow aspiration ↓Platelets Anemia of alcoholism abnormal cellsCreatinine, E.S.R., serum iron IBC B.M aspiration Endocrinal manifestation:
Aregenerative Non Microcytic Anemia Creatinine, E.S.R., serum iron IBC Endocrinal manifestation: A B C Anemia of renal failure Endocrinal manifestation Iron ↓ , ↓ TIBC H. assay: + Fever= e.g., myxoedema Infl. Anemia or panhypopituitrism If –ve A, B, C Do marrow aspiration
Indications of B.M aspiration (In aregenerative non microcytic Anemias) A-if no apparent cause (No R.F, inflammation, Endocrinal manifestation) and no cause of hemodilution ( huge splenomegaly; abn. Ig. Or oedema measure the red cell mass) B-M.C.V. > 110N3 C- if + Neutropenia ±/ Thrombocytopenia, or if there is abnormal cells
1- No erythroblasts anerythroblastic anemia 2- megaloblasts . megaloblastic anemia 3-abn. cells B.M. infilteration 4- hypocellular marrow 5- Normal marrow 6-Malfornied erythroblasts: Dyserythropoiesis e.g.: -Antimeitotic drugs - Congenital -Refractory anemia Marrow aspiration: the following possibilities:
Marrow Biopsy InfilterationFibrosisAplasticNormal -Metastasis Medullany fibrosis aplastic anemia -CLL -ALL. Anemia with N. B.M -AML. -M.M. -NHL.
AREGENERATIVE MEGALOBLASTIC 1) Search for a cause of folic acid or B 12 deficiency: -malnutrition -malabsorption -gastric resection. -relative deficiency: multipara chronic hemolytic anemias. -defect in utilization:alcoholism antifolic drugs. For confirmation: Measure folic acid & B12 serum
AREGENERATIVE MEGALOBLASTIC • 2) If no evident cause: • Seach for pernicious anemia • *schilling test • *gastric acidity test + gastric endoscopy • *folic and B12 serum levels • If low B12,normal folic acid,+ve schilling= • Pernicious anemia
AREGENERATIVE MEGALOBLASTIC • If not pernicious anemia: • we have the following possibilities: • -low B12, N. folic= may be diphylobothrium L • -low folic acid----> do malabsorption tests • -N. B12 and folic----->refractory anemia