Download
1 / 55
800 likes | 1.37k Views
Critical Congenital Heart Disease in the Newborn: Anatomy, Physiology and Surgical Management. Bradley S. Marino, MD, MPP, MSCE

E N D
Critical Congenital Heart Disease in the Newborn: Anatomy, Physiology and Surgical Management Bradley S. Marino, MD, MPP, MSCE Associate Professor of PediatricsStaff Cardiac Intensivist, Cardiac Intensive Care UnitThe Divisions of Cardiology and Critical Care MedicineCincinnati Children’s Hospital Medical Center University of Cincinnati College of Medicine
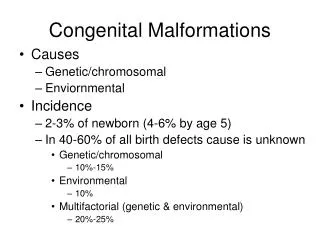
Background • Congenital Heart Disease 8/1000 live births • “Critical” CHD 3/1000 live births • Death • - Cardiac catheterization • - Surgery
Scope of the Problem • In the USA: • ~ 32,000 children born/year with CHD • ~ 11,000/year with “Critical” CHD • ~ 150,000 children in US school system with “repaired” CHD
CHD Presenting in the Neonatal Period 0-6 days 7-13 days 14-28 days (n=1603)(n=311)(n=306) TGA (15%) Coarct (20%) VSD (18%) HLHS (12%) VSD (14%) TOF (17%) TOF (8%) HLHS (9%) Coarct (12%) Coarct (7%) TGA (8%) TGA (10%) VSD (6%) TOF (7%) PDA (5%) Other (52%) Other (42%) Other (38%)
Clinical Presentation of CHD in the Neonate • Fetal Diagnosis • Cyanosis • CHF/Shock/Circulatory Collapse • Arrhythmia • Asymptomatic Heart Murmur
Clinical Presentation of CHD in the Neonate Timing and Symptoms depend on (1) anatomic defect (2) in utero effects (if any) (3) physiologic changes – transitional circulation closure of the ductus arteriosus and fall in pulmonary vascular resistance
Newborn Presentation of CHD • Cyanosis • - Usually minimal symptoms • - First 48-72 hours of life • - Duct-dependent pulmonary blood flow • - Mixing lesion: • TGA, TAPVC, Truncus Arteriosus • CHF/Circulatory Collapse/Shock • - First 2 weeks of life • - Duct-dependent systemic blood flow • - Secondary end-organ dysfunction • Heart, Brain, Kidneys, GI
Evaluation of the Cyanotic Neonate • Cyanosis occurs if there is >3.0g/dL of deoxygenated hemoglobin: • ambient lighting • skin color • hemoglobin; for O2 saturation of 80% • if Hg is 20 gm/dl; 4 gm desaturated-visible cyanosis • if Hg is 10 gm/dl; 2 gm desaturated-not cyanotic • Hyperoxia Test to Determine Intrapulmonary vs. Intracardiac Shunt
Neonatal Presentation-Cyanosis Hyperoxia Test • Room air (if tolerated) • pO2 directly measured or TCOM • 100% FIO2 - “blow-by”, mask, intubated • Repeat mesurement of pO2 right radial artery • Must note site of measurement • Pulse oximetry not acceptable
Hyperoxia Test - Interpretation • pO2 < 100; cyanotic CHD likely • pO2 100-250; cyanotic CHD possible • pO2 > 250; cyanotic CHD unlikely • A “failed” hyperoxia test is a neonatal emergency - urgent intervention.
CHD in the Neonate - Cyanosis • For PO2<50 there is a limited number of • diagnoses possible • Chest Xray VERY Helpful • Massive Cardiomegaly = Ebstein’s Anomaly • Pulmonary Edema = TAPVC • Increased PBF = d-TGA with IVS • Decreased PBF right sided obstructive • lesion with intracardiac R to L shunting
CHD in the Neonate - CyanosisPO2<50 with Decreased PBF • ECG and Cardiac Exam Tricuspid Atresia with PS vs Tricuspid Atresia/Pulmonary Atresia Tetralogy of Fallot vs Tetralogy of Fallot/Pulmonary Atresia Pulmonary Stenosis vs Pulmonary Atresia with IVS
Cyanotic Congenital Heart Disease “Right Sided” Early Presentation
VSD-PS; if severe- may require open PDA for PBF
Ebstein’s Anomaly • In-utero TR • hydrops • SVT common • Sub PS from TV • tissue • iNO helpful to lower • PVR and encourage • antegrade PBF
Pulmonary Atresia-Intact Ventricular Septum • Suprasystemic RV • pressure • TR • CoronarySinusoids
RV-Coronary Connections in PA-IVS
“Critical” Pulmonary Stenosis -“Duct-Dependant” PBF -Non-compliant RV -RL atrial shunt through ASD or PFO
- Anterior • Malalignment VSD • - Aortic Override • - Sub PS • - RVH • 25% 22q11 • Microdeletion
Tetralogy of Fallot- Anterior MalalignmentVSD
Truncus Arteriosus • Conotruncal Defect • VSD • Abnormal Truncal Valve • Single Great Artery • Gives Rise to: • coronary arteries • pulmonary arteries • brachiocephalic arteries • 35% 22q11 Microdeletion
Profound hypoxemia • Low pO2 • High pCO2 • -Shock in the first 48 hours • CXR-small heart, white lungs
Supracardiac TAPVR Lateral Angiogram
Survival Dependant Upon Mixing Between Systemic and Pulmonary Circuits • (PFO, VSD, PDA) • - 40% with VSD • - PDA PGE1 • Balloon Atrial • Septostomy in most • cases of TGA/IVS
Clinical Presentation of CHD in the Neonate • Cyanosis • Congestive Heart Failure • Asymptomatic Heart Murmur • Arrhythmia
Congestive Heart Failure • Clinical Syndrome marked by inability of the heart to meet the metabolic demands of the body • After the first 24-48 hours of life, the neonate with CHF/shock has duct-dependent, left-sided heart disease until proven otherwise • Coarctation of the Aorta • Interrupted Aortic Arch • Critical Aortic Stenosis • Hypoplastic Left Heart Syndrome (HLHS)
Congestive Heart Failure • CHF may be the result of: • Increased demand • - volume or pressure overload • Normal demand but decreased • function • - Inflammatory or metabolic • disease
CHF/Shock in the Neonate • Evaluation for and treatment of • presumptive sepsis should be • undertaken simultaneously.
Upon Closure of PDA: - acute LV afterload - gut, renal perfusion - CHF and acidosis
Posterior Malalignment VSD: • Sub-Aortic Stenosis • - 75% 22q11 Microdeletion
Interrupted Aortic Arch AP View Lateral View Restrictive PDA
LV dysfunction in utero • Endocardial • Fibroelastosis (EFE) • PDA necessary for • systemic perfusion • PFO necessary for • PV return to reach • systemic circulation
1/5000 Live Births Lower Body, CNS and Coronaries Dependant Upon Patent Ductus
Profound CHF-Shock Upon • Ductal Closure • NEC • Hypoxic-Ischemic • CNS Damage • Myocardial Failure
CHF/Shock--Metabolic Acidosis Usually due to decreased tissue perfusion rather than hypoxemia Multifactorial - closing PDA, myocardial dysfunction, shunting of systemic circulation into lungs Treatment: NaHCO3/Inotropic Support/Sedation/Paralysis PGE1
SVC atrial RA LA IVC septum pv SINGLEVENT LV PA LUNGS (PVR) BODY (SVR) PDA-Ao Qs Qp Physiology of HLHS
Critical CHD Is Suspected • Hyperoxia Test indicates Cyanotic CHD (Ductal Dependent PBF) or Shock >48 hours of age (Ductal Dependent SBF) – Heart Disease Likely • - PGE1 0.05-0.1 mcg/kg/min • - Observe 20-30 minutes • - Repeat ABG and Vital Signs • - Umbilical lines
Side Effects of PGE-1 By Birth Weight <2 >2 KG KG ______________________________________ CV 37% 17% CNS 16 16 Respiratory 42 10 Metabolic 5 2 Infectious 11 2 GI 11 3 Hematologic 5 2 Renal 0 2
Prostaglandin E1 • Apnea • Vasodilation/Hypotension • Fever • Seizures (rare) • May “unmask” CHD with obstruction to PV return • TGA with intact atrial septum • TAPVR • Mitral atresia with small PFO (DORV/MA, HLHS)
Supplemental O2 in Critical CHD • Oxygen is a potent pulmonary vasodilator • In lesions with duct-dependant systemic or • pulmonary blood flow (~80% of critical CHD) • Lowering PVR “steals” systemic cardiac • output through PDA • PBF increases at the expense of SBF • As systemic oxygen saturation increases, • systemic oxygen deliverydecreases
Supplemental O2 in Critical CHD • If systemic cardiac output is normal • If hemoglobin and O2 consumption are normal • An oxygen saturation of ~75-85% provides • adequate oxygen delivery to prevent metabolic • acidosis • Titrate supplemental O2 to saturation ~ 80%
Perioperative Management • Initial Stabilization • Airway management • Vascular Access • Newborns-maintenance of PDA • Echocardiographic Diagnosis • Evaluation and Treatment of Secondary Organ Dysfunction • Cardiac Catheterization, if necessary • Surgical Management
The Neonate with Critical CHDEchocardiography • Anatomic and Physiologic Assessment • Serial Changes • Not “Non-Invasive” • - Temperature Instability • - Subcostal View • - Suprasternal Notch View - ? Airway Compromise • - Time Consuming