Download
1 / 97
990 likes | 1.37k Views
Intensifying glycaemic control in Type 2 diabetics. Dr Miriam Blackburn Staff Specialist The Canberra Hospital. Outline. Hba1c Targets Guidelines for intensifying glycaemic control Bariatric surgery Oral hypoglycaemic agents Side effects and PBS listing Starting Byetta

E N D
Intensifying glycaemic control in Type 2 diabetics Dr Miriam Blackburn Staff Specialist The Canberra Hospital
Outline • Hba1c Targets • Guidelines for intensifying glycaemic control • Bariatric surgery • Oral hypoglycaemic agents • Side effects and PBS listing • Starting Byetta • Starting Insulin • Summary
Australian Diabetes Association GuidelinesHba1c target summary • Hba1c goal for most diabetics <7% • More intensive targets • Women planning pregnancy <6% • Requiring lifestyle modification ±metformin • Hba1c ≤ 6.0 % • Requiring any oral antidiabetic agents other than metformin or insulin • Hba1c ≤ 6.5 % • ? Risk of hypoglycaemia with sulphonylureas
Australian Diabetes Association guidelines for Hba1c targets • Hba1c target of <8% • Elderly life expectancy, less than 10 years • Advanced cardiac or renal failure • CKD stage 4 or 5 • NYHA cardiac failure stage 3 or 4 (GFR<30 mls/min) • Incurable malignancy • Moderate Dementia • Hypoglycaemic unaware
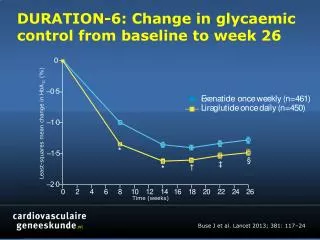
UKPDS 3867 patients with a new diagnosis (treatment naive) of Type 2 diabetes Randomised to intensive therapy (either metformin, sulphonylurea or insulin) or conventional treatment with diet Mean Hba1c of less than 7% in the first five years of the trial for the intensive group Tight glycaemic control was later lost
UKPDS • Patients in the intensive treatment group for the first five years • Significant reductions in microvascular complications, myocardial infarction and death from any cause • Despite loss of the tight control the benefit endured for the next ten years
UKPDS Legacy effect12% reduction in any diabetes related endpoint for patients who had intensive glycaemic control for the first five years
The Legacy EffectAre we meeting the Hba1c guidelines? 60% of Australian patients are not meeting Hba1c targets Clinical inertia/patient compliance
Case History • Mike, a 65 year old Type 2 diabetic • Complicated by mild diabetic retinopathy, no other comorbidities • Medications • Metformin 2 grams daily • Diamicron MR 120 g daily • Tried Byetta (unable to tolerate due to nausea) • Declining bariatric surgery • Hba1c 7.8%, weight 100kg • How would you manage this patient?
Starting Basal Insulin in a Type 2 Diabetic • Add basal insulin 10 units daily of Protaphane or Lantus • Or Add once daily premixed insulin • Novomix 30 10 units with dinner • Increase dose by 2-4 units until fasting BSL 4-7 mmol/L • 0.2 units per kg/day is a reasonable starting dose for add on basal insulin
Intensifying Glycaemic Control for Type 2 Diabetics The traditional way Step 1 Diet and Exercise Step 2 Metformin Step 3 Metformin plus a sulphonylurea Step 4 Metformin plus a sulphonylurea plus a glitazone Step 4 Insulin
Intensifying glycaemic control for Type 2 diabeticsA new approach • Step 1 • Diet and Exercise plus Metformin • Step 2 • Dual therapy • Metformin plus a Sulphonylurea • DPPIV inhibitor plus either a Sulphonylurea or Metformin • Byetta and Metformin or a Sulphonylurea • Step 3 • Triple therapy • Consider Byetta plus Metformin and a sulphonylurea • Step 4 • Insulin +/- oral hypoglycaemic agents
Comparing sulphonylureas and DPPIV inhibitors and GLP1 agonists (Byetta)
Expected Reduction in Hba1c DPPIV inhibitors 0.5-0.8% Byetta 1% Metformin 1-2% Sulphonylurea 1-2% Insulin 1.5-3.5%
Case History • Carol, 45 year old Type 2 diabetic • no complications • Comorbidities • OSA, GORD, OA (waiting TKR) • Medications • Metformin 2 grams daily, Diamicron MR 120 mg daily, Byetta 10mcg bd s/c, Crestor 20 mg daily, Perindopril plus 5mg/1.25 mg, Amlodipine 5mg, Aspirin 100mg
Case History Weight 120kg, BMI 45 Hba1c 9% Had dietician and exercise physiologist review and lost 4kg in 6/12 then gained 6kg in the next 6/12 What is the next step?
Management Refer for bariatric surgery In the meantime, cease Byetta Continue Metformin and Diamicron and start insulin Novomix 30 24 units with dinner or Lantus 24 units before bed (based on 0.2 units per kg) Titrate insulin to get before breakfast sugar between 4-7mmol/L
Indications for bariatric surgery • Failed weight loss by lifestyle change • At least one year of determined effort • BMI>40 • BMI>35 and severe comorbidities • Diabetes, severe osteoarthritis, obstructive sleep apnoea, obesity related cardiomyopathy • Motivated and informed • Canberra Bariatric holds patient information sessions
Gastric SleeveTubular stomach, has fewer ghrelin producing cells
Effects of Bariatric Surgery Mean weight loss 61% Diabetes resolved 77% Hyperlipidaemia improved 70% Hypertension resolved 62% Obstructive sleep apnoea resolved 86% Gastroesophageal reflux symptoms improved Mortality due to operative complications less than 1%, adverse events 20% 30% reduction in mortality due to a reduction in the comorbidities (less cancer, IHD and diabetes related deaths)
Complications of Gastric Banding • Restrictive procedure • Easily reversible • Lowest mortality rate of all bariatric procedures (0.05%) • High rate of revision surgery required (40-50%) • Complications • Acute stomal infection, band infection, haemorrhage, pulmonary emboli, band erosion, band slippage, prolapse or tubing malfunction
Complications of Sleeve Gastrectomy • Lower rate of complications than gastric bypass • Mortality 0.39% • Common complications (3-24%) • Bleeding • Narrowing or stenosis of gastric stoma • Gastric leaks • Reflux
Costs of Bariatric Surgery • If patient has private health insurance • $6000-$7000 out of pocket • If patient has no private health insurance • $19000-20000 • Public funding coming soon…. • Limited number • Strict criteria for eligibility
Case History • Jan, 45 year old • Type 2 diabetes • Diabetes for 10 years • Insulin for 4 years • No complications • Medications • Metformin 2 grams daily • Diamicron MR 120 mg daily • Lantus 30 units nocte
Case History Hba1c 8% Fasting sugar readings 5-6 mmol/L Weight 98 kg, BMI 33 How would you treat this patient?
Management of a Type 2 Diabetic not meeting Hba1c targets on Basal Insulin • Stop Diamicron • Stop sulphonylureas when short acting insulin started • Continue Metformin • To assist with prevention of insulin associated weight gain • Start twice daily pre-mixed insulin • Novomix 30 20 units morning and 10 units at night
Antihyperglycaemic Agents Mechanism of actionSide effectsPBS criteria
ThiazolidinedionesRosiglitazone (Avandia) and Pioglitazone (Actos) • Side effects • Weight gain • Congestive cardiac failure • Osteoporosis and fractures • Rosiglitazone (Avandia) • Boxed warning • Increased risk myocardial infarction and congestive cardiac failure • Adverse effect on lipids • Pioglitazone (Actos) • Increased risk of bladder cancer
Acarbose (Glucobay) • Inhibit upper gastrointestinal enzymes (alphaglucosidases) and slow the absorption of carbohydrate • Side effects • 73% flatulence • Diarrhoea • Compliance maybe poor due to side effects
DPPIV inhibitors SITAGLIPTIN (Januvia)Saxagliptin (Onglyza)Linagliptin (Trajenta)Vildagliptin (GALVUS)
How do DPPIV Inhibitors Work?The Incretin Effect An oral dose of glucose causes more insulin secretion than the same dose given intravenously Glucose in the gut stimulates release of incretins (Glucagon like peptide 1, GLP1 and gastric inhibitory polypeptide, GIP) which increase insulin secretion Patients with diabetes produce less incretins
How do DPPIV inhibitors work? Dipeptidyl peptidase 4 (DPPIV) is an enzyme which metabolises incretins DPPIV inhibitors inhibit DPPIV and cause higher incretin levels This increases insulin secretion and lowers glucose levels Glucose dependant increase in incretin levels therefore no risk of hypoglycaemia (when used as a single agent or with Metformin)
DPPIV Inhibitors Modest effect on Hba1c approximately 0.5% reduction Agents within this drug class have similar efficacy No long term safety data Expensive Weight neutral No risk of hypoglycaemia (unless combined with agents that cause hypoglycaemia e.g. sulphonylurea)
Side effects of DPPIV Inhibitors • Well tolerated • Immune function • Small increased risk of nasopharyngitis, urinary tract infections and headache • Slight increased risk of gastrointestinal side effects with sitagliptin • Linagliptin rare reports of LFT abnormalities (monitor LFT 3/12) • Reports of hypersensitivity reactions • Anaphylaxis, angioedema, Stephen Johnsons syndrome • Pancreatitis case reports • Avoid using if history of pancreatitis or risk factors for pancreatitis (gallstones, severe hypertriglyceridaemia or alcoholism) • Consider pancreatitis if severe abdominal pain develops
Incretin Associated Pancreatitis • Retrospective analysis • Incidence of acute pancreatitis • Control group • Type 2 diabetics not on (DPPIV inhibitors or GLP1 agonists) • 2.7 per thousand developed pancreatitis • Type 2 diabetics taking DPPIV inhibitors or GLP1 agonists • 4.1 per thousand developed pancreatitis
Incretin Associated Pancreatitis Type 2 diabetes increase the risk of pancreatitis two fold Acute pancreatitis increases the risk of pancreatic cancer ?Incretin associated pancreatitis increase the risk of pancreatic cancer Need large scale prospective randomised controlled trials to clarify these questions
PBS requirements for DPPIV inhibitorsLinagliptin, Sitagliptin, Vildagliptin and Saxagliptin Streamlined authority Dual oral combination therapy with metformin or a sulfonylurea and Hba1c>7% Type 2 diabetes where a combination of metformin and a sulfonylurea is contraindicated or not tolerated and Hba1c>7%
PBS requirements for DPPIV inhibitors Private script if used as a single agent Private script if used as triple therapy with Metformin and Sulphonylurea Not to be used with insulin
Comparing DPPIV inhibitors • Linagliptin (Trajenta) • Once daily, one dose 5mg • No dose adjustment required in renal impairment • Saxagliptin (Onglyza) • Once daily • 2.5 mg and 5 mg • Cease if eGFR<60mls/min • Sitagliptin (Januvia) • Twice daily • Dose adjust with renal impairment • Janumet (combination with Metformin) • Vildagliptin (Galvus) • Once or twice daily • Cease if moderate renal impairment • Galvumet (combination with Metformin)