Download
1 / 1
10 likes | 190 Views
CONTINUOUS VERSUS INTERRUPTED SUTURES FOR REPAIR OF EPISIOTOMY AMONGST PRIMIGRAVIDAE Ferry Lee, Ani Amelia Zainuddin , Nur Azurah Abdul Ghani , Zainul Rashid Md Razi .

E N D
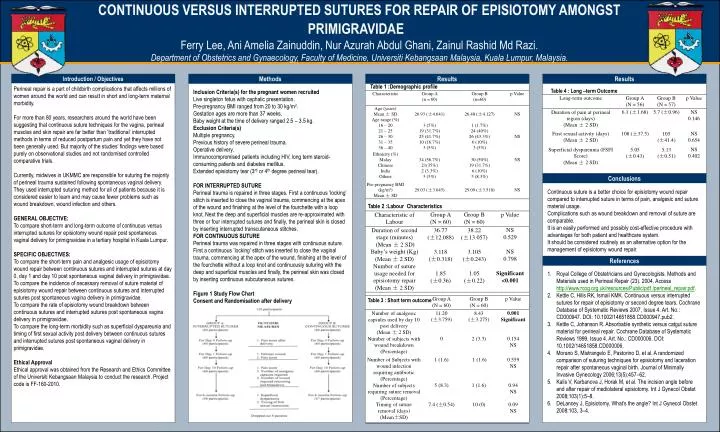
CONTINUOUS VERSUS INTERRUPTED SUTURES FOR REPAIR OF EPISIOTOMY AMONGST PRIMIGRAVIDAE Ferry Lee, Ani Amelia Zainuddin, NurAzurah Abdul Ghani, Zainul Rashid MdRazi. Department of Obstetrics and Gynaecology, Faculty of Medicine, UniversitiKebangsaan Malaysia, Kuala Lumpur, Malaysia. OPTIONALLOGO HERE Introduction / Objectives Methods Results Results Table 1 :Demographic profile • Inclusion Criteria(s) for the pregnant women recruited • Live singleton fetus with cephalic presentation. • Pre-pregnancy BMI ranged from 20 to 30 kg/m2. • Gestation ages are more than 37 weeks. • Baby weight at the time of delivery ranged 2.5 – 3.5 kg. • Exclusion Criteria(s) • Multiple pregnancy. • Previous history of severe perineal trauma. • Operative delivery. • Immunocompromised patients including HIV, long term steroid-consuming patients and diabetes mellitus. • Extended episiotomy tear (3rd or 4th degree perineal tear). • FOR INTERRUPTED SUTURE • Perineal trauma is repaired in three stages. First a continuous ’locking’ stitch is inserted to close the vaginal trauma, commencing at the apex of the wound and finishing at the level of the fourchette with a loop knot. Next the deep and superficial muscles are re-approximated with three or four interrupted sutures and finally, the perineal skin is closed by inserting interrupted transcutaneous stitches. • FOR CONTINUOUS SUTURE • Perineal trauma was repaired in three stages with continuous suture. First a continuous ’locking’ stitch was inserted to close the vaginal trauma, commencing at the apex of the wound, finishing at the level of the fourchette without a loop knot and continuously suturing with the deep and superficial muscles and finally, the perineal skin was closed by inserting continuous subcutaneous sutures. • Figure 1 Study Flow Chart • Consent and Randomisation after delivery • Perineal repair is a part of childbirth complications that affects millions of women around the world and can result in short and long-term maternal morbidity. • For more than 80 years, researchers around the world have been suggesting that continuous suture techniques for the vagina, perineal muscles and skin repair are far better than ’traditional’ interrupted methods in terms of reduced postpartum pain and yet they have not been generally used. But majority of the studies’ findings were based purely on observational studies and not randomised controlled comparative trials. • Currently, midwives in UKMMC are responsible for suturing the majority of perineal trauma sustained following spontaneous vaginal delivery. They used interrupted suturing method for all of patients because it is considered easier to learn and may cause fewer problems such as wound breakdown, wound infection and others. • GENERAL OBJECTIVE: • To compare short-term and long-term outcome of continuous versus interrupted sutures for episiotomy wound repair post spontaneous vaginal delivery for primigravidae in a tertiary hospital in Kuala Lumpur. • SPECIFIC OBJECTIVES: • To compare the short-term pain and analgesic usage of episiotomy wound repair between continuous sutures and interrupted sutures at day 0, day 1 and day 10 post spontaneous vaginal delivery in primigravidae. • To compare the incidence of necessary removal of suture material of episiotomy wound repair between continuous sutures and interrupted sutures post spontaneous vagina delivery in primigravidae. • To compare the rate of episiotomy wound breakdown between continuous sutures and interrupted sutures post spontaneous vagina delivery in primigravidae. • To compare the long-term morbidity such as superficial dyspareunia and timing of first sexual activity post delivery between continuous sutures and interrupted sutures post spontaneous vaginal delivery in primigravidae. • Ethical Approval • Ethical approval was obtained from the Research and Ethics Committee of the UniversitiKebangsaan Malaysia to conduct the research. Project code is FF-160-2010. … Table 4 : Long –term Outcome Conclusions Continuous suture is a better choice for episiotomy wound repair compared to interrupted suture in terms of pain, analgesic and suture material usage. Complications such as wound breakdown and removal of suture are comparable. It is an easily performed and possibly cost-effective procedure with advantages for both patient and healthcare system. It should be considered routinely as an alternative option for the management of episiotomy wound repair. Table 2 :Labour Characteristics References • Royal College of Obstetricians and Gynecologists. Methods and Materials used in Perineal Repair (23). 2004. Access http://www.rcog.org.uk/resources/Public/pdf /perineal_repair.pdf. • Kettle C, Hills RK, Ismail KMK. Continuous versus interrupted sutures for repair of episiotomy or second degree tears. Cochrane Database of Systematic Reviews 2007, Issue 4. Art. No.: CD000947. DOI: 10.1002/14651858.CD000947.pub2. • Kettle C, Johanson R. Absorbable synthetic versus catgut suture material for perineal repair. Cochrane Database of Systematic Reviews 1999, Issue 4. Art. No.: CD000006. DOI: 10.1002/14651858.CD000006. • Morano S, Mistrangelo E, Pastorino D, et al. A randomized comparison of suturing techniques for episiotomy and laceration repair after spontaneous vaginal birth. Journal of Minimally Invasive Gynecology 2006;13(5):457–62. • Kalis V, Karbanova J, Horak M, et al. The incision angle before and after repair of mediolateral episiotomy. Int J GynecolObstet 2008;103(1):5–8. • DeLancey J, Episiotomy, What’s the angle? Int J GynecolObstet 2008:103, 3–4. Table 3 : Short term outcome