Download
1 / 1
10 likes | 70 Views
Results of state policy change to place clients in more appropriate treatment settings Stevens-Manser, S 1 , Arocena, M 2 , Wanser, D 2 , and Spence, R 1 University of Texas, Addiction Research Institute 1 , Texas Department of State Health Services 2. Introduction. Methods. Results.

E N D
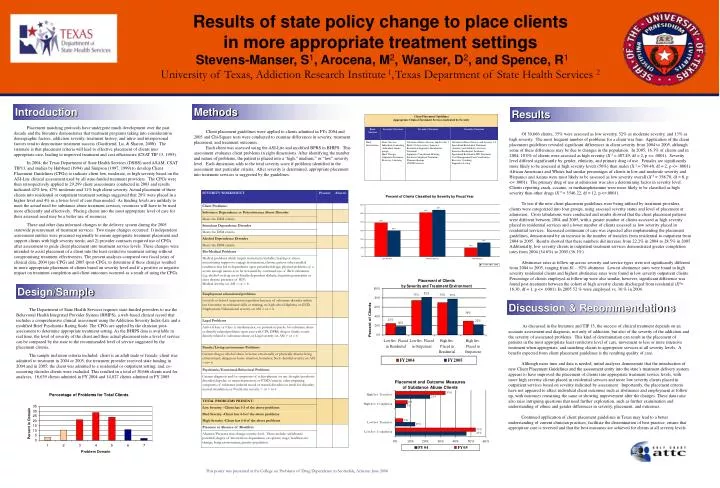
Results of state policy change to place clients in more appropriate treatment settings Stevens-Manser, S1, Arocena, M2, Wanser, D2, and Spence, R1 University of Texas, Addiction Research Institute 1,Texas Department of State Health Services 2 Introduction Methods Results Placement matching protocols have undergone much development over the past decade and the literature demonstrates that treatment programs taking into consideration demographic factors, addiction severity, treatment history, and intra- and interpersonal factors tend to demonstrate treatment success (Gastfriend, Lu, & Sharon, 2000). The rationale is that placement criteria will lead to effective placement of clients into appropriate care, leading to improved treatment and cost efficiencies (CSAT TIP 13, 1995). In 2004, the Texas Department of State Health Services (DSHS) used ASAM, CSAT TIP13, and studies by Hubbard (1994) and Simpson (1997, 1999) to develop Client Placement Guidelines (CPGs) to indicate client low, moderate, or high severity based on the ASI-Lite clinical assessment used by all state-funded treatment providers. The CPGs were then retrospectively applied to 29,299 client assessments conducted in 2003 and results indicated 42% low, 47% moderate and 11% high client severity. Actual placement of these clients into residential or outpatient treatment settings suggested that 20% were placed in a higher level and 4% in a lower level of care than needed. As funding levels are unlikely to meet the actual need for substance abuse treatment services, resources will have to be used more efficiently and effectively. Placing clients into the most appropriate level of care for their assessed need may be a better use of resources. These and other data informed changes to the delivery system during the 2005 statewide procurement of treatment services. Two major changes occurred: 1) independent assessment entities were procured regionally to ensure appropriate treatment placement and support clients with high severity needs; and 2) provider contracts required use of CPGs after assessment to guide client placement into treatment service levels. These changes were intended to assist placement of a client into the least restrictive treatment setting without compromising treatment effectiveness. The present analyses compared two fiscal years of clinical data, 2004 (pre-CPG) and 2005 (post-CPG), to determine if these changes resulted in more appropriate placement of clients based on severity level and if a positive or negative impact on treatment completion and client outcomes occurred as a result of using the CPGs. Client placement guidelines were applied to clients admitted in FYs 2004 and 2005 and Chi-Square tests were conducted to examine differences in severity, treatment placement, and treatment outcomes. Each client was assessed using the ASI-Lite and modified BPRS in BHIPS. This assessment evaluates client problems in eight dimensions. After identifying the number and nature of problems, the patient is placed into a ‘high,” medium,” or “low” severity level. Each dimension adds to the total severity score if problems identified in the assessment met particular criteria. After severity is determined, appropriate placement into treatment services is suggested by the guidelines. Of 30,666 clients, 35% were assessed as low severity, 52% as moderate severity, and 13% as high severity. The most frequent number of problems for a client was four. Application of the client placement guidelines revealed significant differences in client severity from 2004 to 2005, although some of these differences may be due to changes in the population. In 2005, 16.3% of clients and in 2004, 10.0% of clients were assessed as high severity (X 2 = 407.49, df = 2, p <= .0001). Severity level differed significantly by gender, ethnicity, and primary drug of use. Females are significantly more likely to be assessed at high severity levels (56%) than males (X 2 = 769.40, df = 2, p <= .0001). African Americans and Whites had similar percentages of clients in low and moderate severity and Hispanics and Asians were most likely to be assessed as low severity overall (X 2 = 358.70, df = 8, p <= .0001). The primary drug of use at admission was also a determining factor in severity level. Clients reporting crack, cocaine, or methamphetamine were more likely to be classified as high severity than other drugs (X 2 = 3546.22, df = 12, p <=.0001). To test if the new client placement guidelines were being utilized by treatment providers, clients were categorized into four groups, using assessed severity status and level of placement at admission. Cross tabulations were conducted and results showed that the client placement patterns were different between 2004 and 2005, with a greater number of clients assessed as high severity placed in residential services and a lower number of clients assessed as low severity placed in residential services. Increased continuum of care was expected after implementing the placement guidelines, demonstrated by an increase in the number of transfers from residential to outpatient from 2004 to 2005. Results showed that these numbers did increase from 22.2% in 2004 to 28.5% in 2005. Additionally, low severity clients in outpatient treatment services demonstrated greater completion rates from 2004 (34.6%) to 2005 (36.1%). Abstinence rates at follow up across severity and service types were not significantly different from 2004 to 2005, ranging from 81 – 92% abstinent. Lowest abstinence rates were found in high severity residential clients and highest abstinence rates were found in low severity outpatient clients. Percentage of clients employed at follow up were also similar, however, significant difference was found post-treatment between the cohort of high severity clients discharged from residential (X2= 16.30, df = 1, p <= .0001). In 2005 52 % were employed vs. 36 % in 2004. Design/Sample Discussion & Recommendations The Department of State Health Services requires state-funded providers to use the Behavioral Health Integrated Provider System (BHIPS), a web-based clinical record that includes a comprehensive clinical assessment using the Addiction Severity Index-Lite and a modified Brief Psychiatric Rating Scale. The CPGs are applied by the clinician post-assessment to determine appropriate treatment setting. As the BHIPS data is available in real time, the level of severity of the client and their actual placement into a level of service can be compared by the state to the recommended level of service suggested by the placement criteria. The sample inclusion criteria included: client is an adult male or female; client was admitted to treatment in 2004 or 2005; the treatment provider received state funding in 2004 and in 2005; the client was admitted to a residential or outpatient setting; and, co-occurring disorder clients were excluded. This resulted in a total of 30,666 clients used for analyses, 16,639 clients admitted in FY 2004 and 14,027 clients admitted in FY 2005. As discussed in the literature and TIP 13, the success of clinical treatment depends on an accurate assessment and diagnosis, not only of addiction, but also of the severity of the addiction and the severity of associated problems. This kind of determination can result in the placement of patients in the most appropriate least restrictive level of care, movement to less or more intensive treatment when appropriate, and matching clients to appropriate services at all severity levels. A benefit expected from client placement guidelines is the resulting quality of care. Although more time and data is needed, initial analyses demonstrate that the introduction of new Client Placement Guidelines and the assessment entity into the state’s treatment delivery system appears to have improved the placement of clients into appropriate treatment service levels, with more high severity clients placed in residential services and more low severity clients placed in outpatient services based on severity indicated by assessment. Importantly, the placement criteria have not appeared to affect individual client outcomes such as abstinence and employment at follow up, with outcomes remaining the same or showing improvement after the changes. These data raise also raise intriguing questions that need further exploration, such as further examination and understanding of ethnic and gender differences in severity, placement, and outcomes. Continued application of client placement guidelines in Texas may lead to a better understanding of current clinician practices, facilitate the dissemination of best practice, ensure that appropriate care is received and that the best outcomes are achieved for clients at all severity levels. This poster was presented at the College on Problems of Drug Dependence in Scottsdale, Arizona: June 2006