Download
1 / 16
170 likes | 408 Views
Rapid, Robust and Sustained Antiviral Response with Once-daily (QD) Dolutegravir (DTG, S/GSK1349572), a Next Generation Integrase Inhibitor (INI) in Combination Therapy in Antiretroviral-naïve Adults 48 Week Results from SPRING-1 (ING112276).

E N D
Rapid, Robust and Sustained Antiviral Response with Once-daily (QD) Dolutegravir (DTG, S/GSK1349572), a Next Generation Integrase Inhibitor (INI) in Combination Therapy in Antiretroviral-naïve Adults 48 Week Results from SPRING-1 (ING112276) Jan van Lunzen1, Franco Maggiolo2, Bao Phung3, Olga Tsybakova4, Benjamin Young5,6, Jose Gatell7, Steve Almond8, Marty St Clair9, Cindy Brothers9 and Sherene Min9 on behalf of the extended SPRING-1 team 1University Medical Center, Hamburg-Eppendorf, Germany; 2Ospedali Riuniti de Bergamo, Bergamo, Italy; 3Hôpital Bichat-Claude Bernard, Paris, France; 4AIDS Center, Smolensk, Russian Federation5Rocky Mountain CARES/DIDC, Denver, CO, 6Health Connections International, Amsterdam, Netherlands; 7University of Barcelona, Barcelona, Spain; 8GlaxoSmithKline, Missisauga, Canada and 9RTP, USA
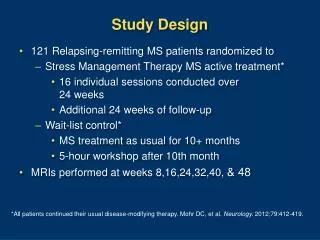
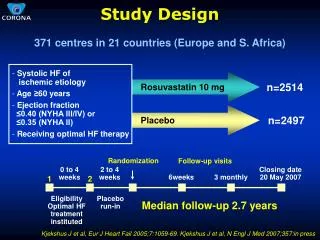
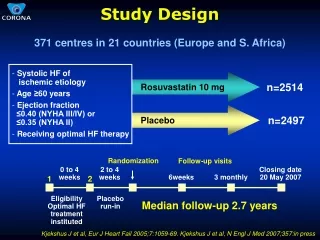
ING112276 Study Design Phase IIb dose-ranging, partially-blinded, N~200 ART-naïve patients All arms include 2 NRTI backbone given once daily Primary endpoint: % <50 c/mL at 16 weeks (TLOVR) Planned interim analysis: % <50 c/mL at 48 weeks (TLOVR) DTG 10 mg 50 mg DTG Selected Dose DTG 25 mg HIV-1 RNA >1000 c/mL CD4 ≥200 cells/mm3 1:1:1:1 Randomization DTG 50 mg • Stratified by • HIV RNA >100,000 • or ≤ 100,000 • Epzicom/Kivexa • or Truvada EFV 600 mg EFV 600 mg Wk 96 Wk 48 interim analysis *Post hoc analysis using bioMONTR HIV-1 EQ SuperLow Assay LLOD=2 c/mLat Weeks 16, 24 and 48
DTG: Rapid and Sustained Antiviral ActivityWeek 48 Efficacy Analysis (%<50 c/mL) 91% 90% 88% 82% Proportion (%) <50 c/mL (TLOVR) DTG 50mg DTG 10mg EFV 600mg DTG 25mg 95% confidence intervals are derived using the normal approximation
Primary Outcomes: % <50 c/mL (TLOVR) at Week 48 *Includes one subject discontinued from study drug due to Burkitt’s lymphoma
Protocol Defined Virologic Failure (>400c/mL) • SPRING-1 (n=150 on DTG) • Week 48, 3/150 (2%) DTG protocol-defined virologic failures (>400 c/mL HIV-1 RNA) • 10 mg DTG, Wk 4: M184V only. No IN mutations or phenotypic changes • 25 mg DTG, Wk 24: 404 c/mL. No geno/pheno determined • 10 mg DTG, Wk 40: No RT, Pro, or IN mutations or phenotypic changes • No subjects in 50 mg arm had confirmed VL >400 c/mL through Wk 48 • No integrase mutations through week 48 • Merck P004 (n=160 on RAL)1 • Week 48, 5/160 (3%) virologic failures (>400 c/mL HIV-1 RNA) • 2/5 (40%) had RAL resistance mutations (N155H) 1. Markowitz, M et al. JAIDS 2007: 46.
50 mg DTG <50 c/mL 600 mg EFV <50 c/mL 50 mg DTG <2 c/mL 600 mg EFV <2 c/mL Response to 50 mg DTG vs 600 mg EFV <50 c/mL and <2 c/mL 100 90 80 70 60 Percent 50 40 30 20 10 0 10 20 30 40 50 60 0 Weeks Abbott RealTime HIV-1 Assay (lower limit ofdetection 40 c/mL) and a modified BioMerieuxEasyQ HIV-1 SuperLow assay (lower limit of detection 2 c/mL)
Median Change from BaselineCD4+ Cell Counts (cells/mm3) Week 24 p=0.008; Week 48 p=0.076Wilcoxon two-sample test, EFV vs. DTG total
AEs (by System Organ Class) Reported in >1 Subject on Investigational Product • No SAEs judged related to DTG • One SAE judged related to EFV (suicide attempt) • No clear dose-response relationship in DTG AEs • Events leading to withdrawal: • DTG (n=2): dyspepsia and Burkitt’s lymphoma • EFV (n=4): abnormal dreams, suicide attempt, drug intolerance, drug hypersensitivity
> Grade 3 lab abnormalities were rare (DTG 12% vs. EFV 14%) No Grade 3 or 4 ALT elevations in any subject Small changes in serum creatinine (0.1 – 0.15 mg/dL) were observed1 Observed with both NRTI backbones, did not progress over time No effect of DTG on GFR (as measured by iohexol clearance) In vitro and clinical data are consistent with inhibition of the renal transporter responsible for tubular secretion of creatinine DTG inhibits the organic anion transporter OCT2 (with IC50 of 1.9 µM), like trimethoprim or cimetidine Laboratory Findings 1. Min S et al. Safety Profile of Dolutegravir (DTG, S/GSK1349572), a Next Generation Integrase Inhibitor (INI) in Combination Therapy in Antiretroviral (ART)-naïve and ART-experienced Adults from Phase 2b Studies. IAS. July 17-20, 2011. Rome. Abstract TUPE238.
DTG Total Chol HDL EFV 600 mg Chol/HDL LDL Trig DTG: Lower Impact on Plasma Lipids than EFV Lipid Parameter -20 -10 0 10 20 30 40 Week 48 Change from Baseline (95% CI) Note: Individual lipids are expressed in mg/dL; Chol/HDL is a unitless ratio.
10 1 0.1 0 5 10 15 20 25 DTG Week 2 Pharmacokinetic Data DTG 10mg once daily DTG 25mg once daily DTG 50mg once daily Mean DTG concentration (ug/mL) PA-IC900.064 ug/mL Post-dose Time (hour) DTG demonstrated low pharmacokinetic variability and drug exposure increased with dose. IQ values ranged 5-19 fold
Conclusions DTG administered once-daily without a PK booster showed a rapid and sustained response at all doses explored through Week 48 No IN resistance mutations detected through 48 weeks DTG was well tolerated with fewer discontinuations than EFV and less impact on lipid parameters Grade 3/4 lab abnormalities were uncommon Small increases in creatinine noted early without progression or safety-related withdrawals1 likely due to non-pathologic inhibition of creatininesecretion These data provide longer term efficacy and safety data for DTG in combination therapy Subjects continue on their randomized regimen until Week 96 1. Min S et al. Safety Profile of Dolutegravir (DTG, S/GSK1349572), a Next Generation Integrase Inhibitor (INI) in Combination Therapy in Antiretroviral (ART)-naïve and ART-experienced Adults from Phase 2b Studies. IAS. July 17-20, 2011. Rome. Abstract TUPE238.
Acknowledgments We thank everyone who has contributed to the success of this study, including: All of our study participants and their families The SPRING-1 Clinical Investigators and their staff: France: J Reynes, L Cotte, F Raffi, C Katlama, P Yeni, J-M Molina Germany: J van Lunzen, H-J Stellbrink, M Stoll, T Lutz Italy: G Carosi, F Maggiolo, G Rizzardini, A Lazzarin Russia: O Tsybakova, E Voronin, A Rakhmanova Spain: F Pulido, J Arribas, S Moreno-Guillen, J Gatell, B Clotet United States: E DeJesus, F Felizarta, T Hawkins, J Lalezari, L McCurdy, G Richmond, S Schneider, L Sloan, J Torres, B Young, T Vanig, M Mustafa, A LaMarca And the extended ViiV Healthcare-Shionogi-GlaxoSmithKline SPRING-1 study team
Laboratory Findings > Grade 3 lab abnormalities were rare (DTG 12% vs. EFV 14%) No Grade 3 or 4 ALT elevations in any subject Changes (+/- SD) in serum creatinine over time Note: no clinically relevant events nor discontinuations related to creatinine See also abstract TUPE238 (Min et. al.)