Download
1 / 25
250 likes | 438 Views
Perceived Contraindications to IUD and Implant Use Among Family Planning Providers. Ashley Philliber, Heather Hirsch, Rita Turner and Susan Philliber Philliber Research Associates. 16 Main Street Accord, NY 12404 845-626-2126 Fax 845-626-3206. Presenter Disclosures. Ashley Philliber.

E N D
Perceived Contraindications to IUD and Implant Use Among Family Planning Providers Ashley Philliber, Heather Hirsch, Rita Turner and Susan Philliber Philliber Research Associates 16 Main Street Accord, NY 12404 845-626-2126 Fax 845-626-3206
Presenter Disclosures Ashley Philliber No relationships to disclose The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months:
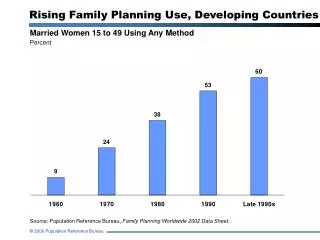
IUD and Implant Use • Effective methods • Convenient • Few complaints about side effects— but still low use 8.5% of women in 2009
IUD and Implant Use • Has risen from 2.4% to 8.5% between 2002 and 2009 • But in China, 41% of women use Norway, 27% of women use
Among patients • New studies show prevention of rapid repeat pregnancies among adolescents (Tocce, Sheeder and Teal, 2012) • High patient satisfaction and thus, high continuation rates (Doyle et al., 2008; Stoddard, McNicholas and Peipert, 2011) So what’s the problem?
Barriers to LARC Use • Cost, cost, and cost --Recent studies show that when the cost barrier is removed, adoption rates rise dramatically (Peipert et al., 2012, PRA and UCSF, 2012) • Cost effective over time but initial cash outlay outstrips a monthly pack of pills
Maybe providers are a problem? • One recent study in SC showed students in a family medicine residency --had limited knowledge about IUD use, and --90% inserted fewer than 10 per year. (Diaz at al., 2011)
Providers may be a problem • Some suggest that providers do not use LARC as the first line methods of choice but instead— --make women “earn” their IUDs after failing with other methods, and --use LARC as methods of “last resort”. (Hubacher, 2002)
Provider Fears • In a study of California’s Family PACT Program --61% had IUDs available at their practices --only 60% felt very comfortable inserting ParaGard® --only 40% felt very comfortable inserting Mirena®
In this paper… • We report data from 159 and 114 providers in family planning clinics in Colorado and Iowa • Part of an evaluation of two Initiatives to Reduce Unplanned Pregnancies • Mostly Title X clinics
The ACOG Guidelines Long-acting reversible contraceptive methods have few contraindications and almost all women are eligible for implants and IUDs. --ACOG Practice Bulletin, 2011, p. 3
Besides this general endorsement, ACOG comments on specific groups The immediate post-partum period is a particularly favorable time for IUD or implant insertion. --ACOG Practice Bulletin, 2011, p. 4
But among these providers… Percentage agreeing that immediate post-partum(prior to discharge) insertion is suitable and safe
Or after an abortion Insertion of an IUD or implant immediately after either an abortion or miscarriage is safe and effective. --ACOG Practice Bulletin, 2011, p. 5
But among these providers… Percentage agreeing that immediate post-abortion(prior to leaving the clinic) insertion is suitable and safe
Or after an ectopic pregnancy Intrauterine devices may be offered to women with a history of ectopic pregnancy. …The contraceptive implant does ot increase the risk of ectopic pregnancy in women with previous history of ectopic pregnancy. --ACOG Practice Bulletin, 2011, p. 6-7
But among these providers… Percentage agreeing that LARC is suitable andsafe for women with a history of ectopic pregnancy
ACOG says Both nulliparious women and adolescents could be offered LARC methods including IUDs. --ACOG Practice Bulletin, 2011, p. 3.
But among these providers… Percentage agreeing that LARC is suitable and safe fornulliparous women and teenagers (ages 15-19) *Difference between 2010 and 2012 is significant at p <.05.
There are some areas of agreement • Both ACOG and these providers approve LARC for— --women with previous STIs --young adults aged 20-29
These are the providers eligible to insert • But among the RNs in our sample— --much more conservative responses --only 7% thought immediate post-partum insertion was suitable and safe --only 73% thought teens could have LARC
So what? • Maybe it just takes time and our data do show improvements between 2010 and 2012 • But national organizations who train these providers need to close this gap • Routine stocking of LARC is needed
So what? • Reimbursement post-partum and post-ab would help • Education of all those doing counseling is necessary
Overall In a nation where almost half our pregnancies are unplanned, these methods are greatly needed. Providers need to see them as the methods of preference on the dimensions of safety, effectiveness, and convenience.
Studies among women • Concerns about safety and long-term infertility • Misunderstanding • Fear of insertion