Download
1 / 31
310 likes | 337 Views
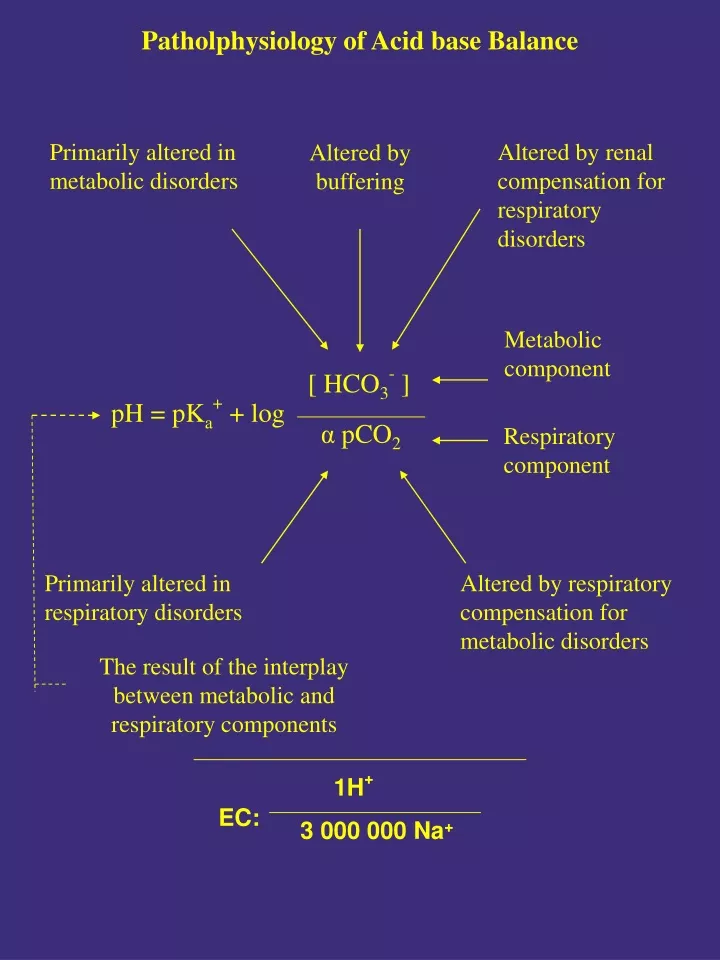
1H + 3 000 000 Na +. EC:. Patholphysiology of Acid base Balance. Primarily altered in metabolic disorders. Altered by renal compensation for respiratory disorders. Altered by buffering. Metabolic component. [ HCO 3 - ]. pH = pK a + + log. α p CO 2. Respiratory component.

E N D
1H+ 3 000 000 Na+ EC: Patholphysiology of Acid base Balance Primarily altered in metabolic disorders Altered by renal compensation for respiratory disorders Altered by buffering Metabolic component [ HCO3- ] pH = pKa+ + log α pCO2 Respiratory component Primarily altered in respiratory disorders Altered by respiratory compensation for metabolic disorders The result of the interplay between metabolic and respiratory components
Extracellular pH 7.4 7.1 6.9 6.7 240 6.7 200 160 Cellular pH Cellular (H+) nmol/l 120 6.9 7.1 80 7.4 40 7.7 80 0 40 120 200 (H+) nmol/l Buffering of Strong Acid added to Extracellular Fluid Compartment Contribution Time course Instantaneous Rapid Slow Min Hrs/days 40% 50% 10% PCO2 HCO-3 Extracellular fluid Cells Bone and connective tissue Physochemical buffering Respiratory Physiological regulation Renal
Cell functions depending on regional pH • Plasma membrane function • - Passive permeability to cations and anions • - Active transport processes • - Hormon receptor functions • - Cell shape, motility and excitability • - Endo- and exocytosis Mitocondrial function - Energy storage - ATP generation - Ammoniagenesis - Other enzyme activities Cytoplasmic function - Glycolysis - Glyconeogenesis - Cyclic nucleotid function - Function of actin and myosin - Cytoskeleton function - O2 affinity of hemoglobin Function of other organelles
Metabolic Acidosis Acidexcess Base loss Gastrointestinal loss of HCO-3 - diarrhea - small- bowel or pancreatic fistula, drainage - ureterosigmoidostomy - anion exchange resins Renal loss of HCO-3 - carbonic anhydrase inhibitors - renal tubular acidosis (RTA) - hyperparathyroidism - hypoaldosteronism Exogen acids: -HCl (fe. arginin chlorid, NH4Cl ) -H2SO4 ( fe. Methionin) Incomplete fat oxidation: -diabetes mellitus (ketoacid) -starvation -alcoholic ketoacidosis Incomplete carbohydrate oxidation: (lactic acidosis) -shock, diabetes -cirrhosis -leukemia Failure of acid excretion: ARF, CRF Ingestion of toxic substances: - salicylate overdose, - methanol, ethylene glycol
Metabolic acidosis Buffering EC IC Bone Compensation Lung: hyperventillation pCO2 = 1,0 1,5* (HCO-3) (CO2 =34-31 mmHg 18mmol HCO-3) Kidney: total acid excretion = UNH4 *V+ UTA*VU HCO-3*V 1mmol/kg/day max. ca. 600 mmol/kg/day
Laboratory of Metabolic Acidosis pH , HCO-3 , pCO2 Se-K (ICK ECK: total – K ) Anion gap = Na+ + K+- Cl- - HCO-3 norm: 12-20 mmol/l Na++ K++ Ca++ + Mg++ = Cl-+ HCO-3+ PO=/-4 + organic anions + protein + SO- -4 ~Ø Non measured anions (~ // mmol/l – albumin) AG : (strong acids buffering HCO3 other anions ) Increased acid formation -diabetic ketoacidosis -alcoholic lactic acidosis Toxic materials -salycilate -methanol -ethylen glycol Acid excretion -ARF, CRF AG : (HCO-3 Cl- - reabsorption hypercloremia): Gastrointertinal loss: Renal loss -diarrhea etc. - Carbonic anhydrase inhibitors - pancreatic fistula - Renal tubular acidosis (RTA) - Hyperparathyroidism - Hyperaldosteronism
Failure of Acid Excretion in Renal Disease Daily acid load Diseased kidney Buffering by ECF and intracellular buffers Solute and water load per nephron Bone buffering Nephron population Filtered phosphate Proximal HCO3- reabsorption per nephron Ability to maintain or increase NH3 secretion Urinary buffer (phosphate) Distal HCO3- delivery Plasma HCO3- concentration Complete HCO3- reabsorption Titratable acid excretion relative to degree of acidosis NH4 excretion Urinary HCO3- leak Acid urine Net acid excretion
Respiratory response to metabolic acidosis. The increase in (H+) produced by metabolic acidosis is sensed by chemoreceptors in the brainstem and ventilation is stimulated, reducing PCO2. Altough no units are shown on the time axis, this response is fully manifest in 1 to 3 hours, and the reduction in PCO2 induced is sustained until the bicarbonate deficit is repaired. During the recovery process, a similar delay occurs between correction of the acidosis and restoration of normal ventilation, resulting in a transient period of alkalemia.
Causes of Lactic Acidosis Clinically characterised by decrease in tissue oxigenation No clinical sign of decreased tissue oxigenation Systemic disorders or conditions -diabetes mellitus -liver failure -sepsis -malignancy -pregnancy Intoxication -Ethanol -Etlylenglycol -Strychnine Muscular hyperactivity -seizures -marathon running Cardiogenic shock Hypovolemic shock Septic shock Hypoxemia (O2 < 35mmHg) Anemia ATP NADH Venous constriction Arteriolar dilatation Myocordial contraction Congrestive Heart failure (pH7.10-7.20) lactate mortality If > 4 mmol /l
Lactic Acidosis Decreased lactate metabolism Increased lactic acid production anion gap H+ + lactate HCO3- Distal nephron delivery of lactate (if plasma lactate > 7 to 8 mmol/l) pH Distal nephron anion (lactate) delivery Na+ lacate- excretion Buffering (ECF + ICF) Renal NH3 production ECF volume Ventilation Difference in lumen negative potential Distal nephron Na+ avidity Renal H+ secretion Renal NH4+ excretion Renal TA excretion Generation of HCO3- Generation of HCO3- pCO2 Rise in pH toward normal
Causes of Renal Tubular Acidosis Distal Proximal Hypokalemic or normokalemic - Primary - Hypercalcemia - Nephrocalcinosis - Multiple myeloma - Hepatic cirrhosis - Lupus erythematosus - Amphotericin B - Lithium - Toluene - Renal transplant rejection - Medullary sponge kidney Hyperkalemic - Hypoaldosteronism - Obstructive nephropathy - Sickle cell nephropathy - Lupus erythematosus Primary Cystinosis Wilson’s disease Lead toxicity Cadmium toxicity Mercury toxicity Amyloidosis Multiple myeloma Nephrotic syndrome Early renal transplant injury Medullary cystic disease Outdated tetracycline
Proximal Tubular Acidosis Proximal tubules: HCO-3 reabsorption distal HCO-3 load (norm: 85%) urine HCO-3hypercloremic metabolic alkalosis urine : Na+ , K+ , H2O Hyponatremia, hypokalemia, hypovolemia
NORMAL 25 HCO-3 Reabsorption (meq/L GFR) COMPLETE REABSORPTION 20 PROXIMAL ( Type II) RTA 15 TRESHOLD Plasma (HCO-3) (meq/L) 15 20 25 Filtered load Proximal reabsorption Distal delivery Distal reabsorption Urinary excretion Norm: ~ 80%: ~20 15%: ~ 4-6 60% „4 ~ 6” „6” „8” „10” 15% pH 5.5 pH 6.5 pH 7.8 Bicarbonate titration curve and segmental nephron deliver and absorption in proximal (type II) RTA
6 Proximal RTA (type II): hypokalemic, hyperchloremic metabolic acidosis (in acidosis: net acid excretion = acid generated) HCO3- CO2 H2CO3 CAIV 4 LUMEN 1 H2O 8 CO2 ADP H+ OH- Pi 3 7 PROXIMAL TUBULE CELL Na+ CAIII ATP ADP HCO3- Pi 5 2 BLOOD K+ Pathophysiology of proximal (type II) RTA. The possible causes of abnormal proximal acidification include defects in the luminal Na+-H+ antiporter (1); the basolateral Na+-HCO3- symporter (2); the intracellular (3) or luminal (4) carbonic anhydrases (CA); sodium permeability (5); the Na-K ATPase (6); the intracellular generation of ATP (7); or membrane recycling, metabolism, or trafficking (8).
Pathophysiologic Mechanisms of Distal Renal Tubular Acidosis Defect Mechanism Example Gradient or backleak Secretory Voltage-dependent Rate-dependent Hypoaldosteronism Amphotericin B Classic distal RTA Amiloride, obstructive nephropathy, sickle cell disease Interstitial nephropathy Hyporeninemic hypoaldosteronism Inability to achieve or maintain a low urine pH due to backleak of H+ or H2CO3 Decrease in both force and rate (conductance) of the H+ pump system; acidification impaired under all conditions Failure to maintain a negative potential difference in the collecting duct lumen due to decreased sodium reabsorption Decreased rate of H+ secretion, but intact ability to achieve a low pH with an acid load (force intact) Probably a combination of voltage-dependent and rate-dependent defects and decreased ammonia production
Classical Distal RTA (type I): hypokalemic, hyperchloremic metabolic acidosis (in urine: inappropriate acidification) NH3 NH4+ HPO4 H2PO4- (TA) H+ 3 LUMEN 1 ADP ATP Pi H2O DISTAL TUBULE OH- CA CO2 Cl- HCO3- 2 BLOOD Pathophysiology of classical distal (type I) RTA. The possible causes of abnormal intercalated cell acidification in the distal nephron include defects in the luminal proton-translocating ATPase (1), the basolateral HCO3-Cl- antiporter (2), or luminal hydrogen ion permeability (3). TA, titratable acid; CA, carbonic anhydrase.
Metabolic alkalosis Netto H+ loss (vomiting hyperaldosteronism) Netto HCO-3 increase (milk-alkali syndrome, baking powder) Cl- loss>HCO-3 loss (diureticum) Buffering ( IC+EC) HCO3+ + H+ CO2+H2O Compensation Pulmonary : hypoventillation Max. pCO2 ~ 60 mmHg Kidney: HCO3- secretion Maintaining factors: 1. Hypocloremia prox. tub. HCO-3 – reabs. 2. Hypokalemia „paradox aciduria” 3. Hypovolemia 4. Hyperaldosteronism ΔpCO2=0.25-1.0 *Δ HCO-3 (Fe: pCO2 43-50 mmHg 34mmol/l (HCO-3)
Metabolic alkalosis NASOGASTRIC SUCTION REMOVAL OF WATER POTASSIUM SODIUM HYDROGEN ION CHLORIDE pH PLASMA HCO3- PLASMA AND FILTERED Cl- ECF VOLUME H+ SHIFTS INTO ECF K+ SHIFTS INTO CELLS ALDOSTERONE FILTERED HCO3- HYPOVENTILATION PaCO2 K+ EXCRETION HYPOKALEMIA HCO3-”REABSORPTION” MAINTENANCE OF METABOLIC ALKALOSIS
NaCl-sensitive metabolic alkalosis (f.e.: vomiting) ECV Na+ reabsorption NaCl + Low [Cl-] Urine Cl- < 10 mmol/l HCO3- reabsorption Alkalosis (priority of volumen regulation over the pH)
NaCl resistant metabolic alkalosis (f.e.: glycocorticoid therapy) ECV Proximalis NaClreabsorption NaCl Diastalis Na+ reabsorption H+, K+ excretion HCO3- reabsorption Alkalosis
Differential Diagnosis of Metabolic Alkalosis Sodium chloride-responsive (UCl- <10 mmoles/L) Gastrointestinal disorders Vomiting Gastric drainage Villous adenoma of the colon Chloride diarrhea Diuretic therapy Correction of chronic hypercapnia Cystic fibrosis Sodium chloride-resistant (UCl- < 20 mmoles/L) Excess mineralocorticoid activity Hyperaldosteronism Cushing’s syndrome Bartter’s syndrome Excessive licorice intake Profound potassium depletion Unclassified Alkali administration Recovery from organic acidosis Antacids and exchange resins in renal failure Milk-alkali syndrome Massive blood or Plasmanate transfusion Nonparathyroid hypercalcemia Glucose ingestion after starvation Large doses of carbenicillin or penicillin
Causes of Acute Respiratory Acidosis Neuromuscular abnormalities Brain stem injury High cord injury Guillain-Barré syndrome Myasthenia gravis Botulism Narcotic, sedative, or tranquilizer overdose Airway obstruction Foreign body Aspiration of vomitus Laryngeal edema Severe bronchospasm Thoracic-pulmonary disorders Flail chest Pneumothorax Severe pneumonia Smoke inhalation Severe pulmonary edema Vascular disease Massive pulmonary embolism Respirator-controlled ventilation Inadequate frequency, tidal volume settings Large dead space Total parenteral nutrition (increased CO2 production)
Acute Respiratory Acidosis pCO2 ; pH ; pO2 ; act. HCO3 ; st. HCO3 [HCO3-] = (pCO2/10)3 (f.e.: [HCO3-] 24-30 mmol/l pCO2 70 mmHg (12-24 ))
Causes of Chronic Respiratory Acidosis Neuromuscular abnormalities Chronic narcotic or sedative ingestion Primary hypoventilation Pickwickian syndrome Poliomyelitis Diaphragmatic paralysis Thoracic-pulmonary disorders Chronic obstructive airway disease Kyphoscoliosis End-stage interstitial pulmonary disease Laboratory pCO2 ; pH ; pO2 ; act. HCO3 ; st. HCO3- [HCO3] = 4x pCO2/10 4 (f.e.: [HCO3] 32-40 mmol/l pCO2 70 mmHg)
Respiratory acidosis EFFECTIVE ALVEOLAR VENTILATION CO2 EXCRETION PaCO2 RENAL H+ SECRETION H2CO3 AND pH NH4 EXCRETION BALANCED BY Cl- EXCRETION HCO3 –RECLAMATION AND GENERATION INTRACELLULAR BUFFERS CONSUME H+ NET ACID EXCRETION PLASMA HCOCONCENTRATION APPROPRIATELY DEFENDED CHRONIC RESPIRATORY ACIDOSIS
Figure: Schematic time course of the changes in plasma acid-base equilibrium during the development of respiratory acidosis.
Causes of Respiratory Alkalosis Central stimulation of respiration Anxiety Head trauma Brain tumors or vascular accidents Salicylates Fever Pain Pregnancy Peripheral stimulation of respiration Pulmonary emboli Congestive heart failure Interstitial lung diseases Pneumonia „Stiff lungs” without hypoxemia Altitude Uncertain Hepatic insufficiency Gram-negative septicemia Mechanical or voluntary hyperventilation
Respiratory Alkalosis Acute: [HCO3 -] = 1-3x (pCO2/10) (f.e.: [HCO3 -] 23-21 mmHg pCO2 30 mmHg) Chronic: [HCO3 -] = 2-5x (pCO2/10) (f.e.: [HCO3 -] 22-19 mmHg pCO230 mmHg)
Respiratory alkalosis ALVEOLAR VENTILATION CO2 EXCRETION PaCO2 RENAL H+ SECRETION ECF pH HCO3 RECLAMATION NH4 EXCRETION TA EXCRETION INTRACELLULAR BUFFERS ADD H+ TO ECF BICARBONATURIA NET ACID EXCRETION Na+ K+ EXCRETION PLASMA HCO3 -CONCENTRATION Acute respiratory alkalosis [HCO3-]= 1-3x (pCO2/10) (f.e.: pCO2: 30 mmHg [HCO3-]: 23-21 mmol/l) Chronic respiratory alkalosis [HCO3-]= 2-5x (pCO2/10) (f.e.: pCO2: 30 mmHg [HCO3-]: 22-19 mmol/l)
Mixed Acid-Base Disorders Disorders Compensation pH Type 1: Failure of compensation Metabolic acidosis and respiratory alkalosis PaCO2 too high and [HCO3-] too low for simple disorders PaCO2 too low and [HCO3-] too high for simple disorders Metabolic alkalosis and respiratory alkalosis Type 2: Excessive compensation PaCO2 too low and [HCO3-] too low for simple disorders Normal or slightly or Metabolic acidosis and respiratory alkalosis PaCO2 too high and [HCO3-] too high for simple disorders Normal or slightly or Metabolic alkalosis and respiratory alkalosis
Example of a Triple Acid-Base Disorder Clinical event Acid-base disorder pH PaCO2 (mm Hg) [HCO3-] (mmoles/l) Anion gap (mEq/L) Hyperventilation Respiratory alkalosis 7.46 20 14 34 Vomiting Metabolic alkalosis 7.53 44 36 14 Hypovolemic shock Metabolic acidosis 7.35 30 16 32






















