Download
1 / 40
540 likes | 987 Views
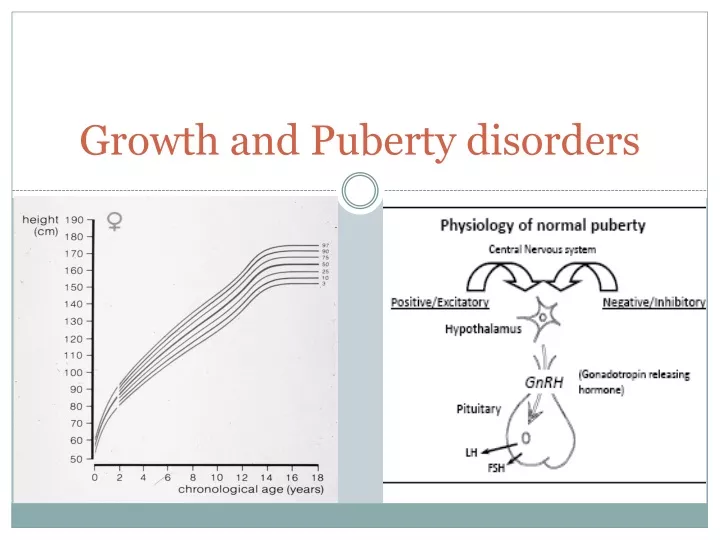
Growth and Puberty disorders. Is she short?. Short stature. Standing height > 2SD below the mean (< 2.5 percentile) for gender and chronological age. Investigation of children <-2SDS identifies pathology in 14%

E N D
Short stature • Standing height > 2SD below the mean (< 2.5 percentile) for gender and chronological age. • Investigation of children <-2SDS identifies pathology in 14% • Investigation of children <-3SDS identifies pathology in 58% • Compare the child’s height with that of a larger population of a similar background and mid-parental target height.
Key points • Short stature is defined as standing height or recumbent length more than 2 standard deviations (SD) below the mean value for chronologic age. • Height (growth) velocity (cm/year) is another key auxological parameter in the assessment of a child for short stature. • Height of a child must always be defined in the context of genetic potential conferred by parental heights. • Short stature must not be confused with failure to thrive.
Height velocity How to measure Ht? • Ideally with calibrated stadiometer • Wall mounted • Tabletop recumbent (length)< 2 yrs old • Children who can’t stand: • Arm span • should approximate the height (>8yrs old)
Most important aspect of growth evaluation Change in standing Ht over: Infants: 4 mo Children: 6mo Normal (cm/yr) 1y: 25 2y: 12 3y: 8 Then until puberty: 4-7 cm Growth velocity
Regulation of postnatal growth • Infancy: – Nutrition – GH/IGF-I • Childhood: – GH/IGF-I – Thyroxine • Pubertal: – GH/IGF-I – Sex steroids
SS Causes 1 • Non-pathogenic – Constitutional Delay of Growth and Puberty – Familial short stature – Nutritional • Intra-Uterine Growth Restriction – Syndromic e.g Silver-Russell syndrome – Non-syndromic • Systemic disorders – Cardiovascular disease e.g. congenital heart disease – Renal e.g. chronic renal failure, RTA – Respiratory e.g. cystic fibrosis, asthma – Gastrointestinal disease e.g. IBD – Neurological e.g. brain tumour – Psychosocial e.g. anorexia nervosa, child abuse
ETIOLOGY OF SHORT STATURE • Constitutional Delay of Growth and Development/Constitutional Delay of Growth and Adolescence
CDGP • Growth velocity may be transiently decreased in the first 2 to 3 years of life (“catch down”) but normal thereafter. In some cases, a decrease in growth velocity occurs just prior to the appearance of secondary sex characteristics. • Delayed skeletal maturation (bone age) and delayed onset of puberty •Height age same as bone age •Final adult height and progression of sexual development are normal. •Often with family history of delayed growth and onset of sexual development
Familial Short Stature • Bone age generally not significantly delayed and often same as chronological age • Normal length and weight at birth
Bone age (skeletal maturation) • Greulich and Pyle (compare epyphiseal centers in hand and wrist)
Nutritional •Caloric insufficiency •Chronic inflammatory bowel disease •Malabsorption •Celiac disease
SS Causes 2: Endocrine causes GH-related causes • Growth hormone (GH) deficiency: isolated or combined with other pituitary hormone Deficiencies • GH insensitivity Hypothyroidism Glucocorticoid excess • Cushing syndrome • Poorly managed congenital adrenal hyperplasia • Exogenous corticosteroid administration Pseudohypoparathyroidism
SS Causes 3: Chromosomal and Genetic causes – Turner syndrome – Noonan syndrome – Down syndrome – Skeletal dysplasias –achondroplasia, hypochondroplasia, spondylo-epiphyseal dysplasia – Seckel syndrome – Prader-Willi syndrome – Miscellaneous other syndromes e.g. Rothmund- Thompson syndrome, Leri-Weill syndrome, Progeria, mucopolysaccharidoses
Chronic Disease • Chronic renal disease • Chronic liver disease • Congenital heart disease • Pulmonary (cystic fibrosis, asthma) • Poorly controlled diabetes mellitus • Anemias (sickle cell or thalassemia)
Chronic Use of Drugs/Medications • Glucocorticoids • High-dosage estrogens • High-dosage androgens • Methylphenidate • Dextroamphetamines
EVALUATION OF SHORT STATURE Prenatal history, including maternal infection, consumption of alcohol or drugs, and smoking Pattern of growth (height and weight), including birth weight and length in relation to gestational age Family history, including parental heights and age of onset of puberty of parents and first-degree relatives Profile of patient’s pubertal development, including age of onset of breast development and menarche, testicular and penile enlargement, pubic hair, and body odor Nutrition
Evaluation of short stature Evidence of systemic disease (gastrointestinal, cardiac, pulmonary, renal) Drug administration (steroids, methylphenidate) Psychosocial milieu Neurologic symptoms, especially headache, visual disturbance
Physical Examination Accurate measurements of height, weight, head circumference, arm span, and upper and lower body segments Assessment of nutritional state and fat distribution Abnormal pigmentation of the skin Dysmorphic features Sexual maturity rating (Tanner staging) Neurological examination including fundoscopy and visual field tests Examination of the thyroid gland
Target height of the child BOYS: [Father’s ht (cm)+ (mother’s Ht (cm)+ 13)] 2 • GIRLS: • [(Father’s ht (cm) -13) + mother’s Ht(cm)] • 2 • Inches: change 13 for 5’’
Baseline investigations for short stature • Full blood count, ESR • Creatinine, urea, electrolytes • Calcium, phosphate, liver function tests • Ferritin, endomysial antibodies • Karyotype (in girls) • T4, TSH • Skeletal survey in dysmorphic children • Bone age X-ray (this is NOT a diagnostic investigation)
Further investigations • Low levels of IGF-1 and IGFBP3 are suggestive of GH deficiency • Provocative GH stimulation test (insulin, arginine, clonidine, glucagon, L-dopa) is the accepted method for confirming the diagnosis of GH deficiency.
FDA-Approved indications for growth hormone therapy • GHD • PWS • SGA/IUGR • Turner syndrome • Noonan syndrome • ISS • Chronic renal insufficiency • AIDS wasting • Adult GHD • SHOX deficiency
Side effects of GH therapy • Hypothyroidism • Edema and sodium retention • Benign intracranial hypertension • Insulin resistance • Slipped capital femoral epiphysis • Scoliosis • Gynecomastia • ???Development of cancers
In which of the following conditions is the BA consistent with chronological age (not delayed)? • Acquired hypothyroidism • Constitutional delay • Familial short stature • Glucocorticoid excess • Psychological dwarfism
You are evaluating a 6yo girl for short stature. Her growth chart reveals a birth length at 60th percentile, and a current height at 5th percentile. Her growth velocity in the last 3 yrs has been 3cm/yr. Her weight is at the 50th percentile. On PE: wnl, and her intelligence appears normal. There are no midline defects or dysmorphic features. Her BA is 4 yrs. What is the most llikely dx? • Congenital hypothiroidism • Crohn disease • GH deficiency • Spondilodysplasia • Turner