Download
1 / 44
460 likes | 648 Views
بسم الله الرحمن الرحيم. CDH Congenital Dislocation of the Hip. Prof. Mamoun Kremli AlMaarefa College. Spectrum of diseases. Abnormality of proximal femur and acetabulum Initial pathology is congenital, but Progresses (becomes worse) if not treated Does not always result in dislocation.

E N D
بسم الله الرحمن الرحيم CDHCongenital Dislocation of the Hip Prof. Mamoun Kremli AlMaarefa College
Spectrum of diseases • Abnormality of proximal femur and acetabulum • Initial pathology is congenital, but • Progresses (becomes worse) if not treated • Does not always result in dislocation
Nomenclature • CDH: Congenital Dislocation of the Hip • DDH: Developmental Dysplasia of the Hip • CDH: Congenital Dysplasia of the Hip • CHD: Congenital Heart Disease!
CDH - Spectrum • Acetabular dysplasia: • Shallow acetabulum • Unstable hip: • Dislocatable - Reducible • Dislocated hip: • May or may not be reducible • Teratologic hip: • Fixed dislocation at birth, often with other major anomalies
Incidence • Hip instability at birth: 0.5 – 1 % • Classic CDH: 0.1% • Mild dysplasia: Substantial • Up to 50%of hip arthritis in ladies have underlying hip dysplasia
Etiology Multi-factorial • Ligament laxity • Genetic • Mechanical factors
Etiology 1. Ligament laxity • Hormonal: • Estrogen, Relaxin: hormones secreted by mothers before birth • May affect baby girls more? – receptors • Familial ligament laxity: • Mild – Moderate – Sever • Ehler Danlos Syndrome
Etiology Ligament laxity: hypermobile joints
Etiology 2. Genetic factors • Twin studies • Monozygotic: 38% • Dizygotic: 3% (similar to other siblings) • Positive family history • Females: 4-6 X more than males • Could be hormonal – the effect of Relaxin hormone produced by mother on female fetus
Etiology 3. Mechanical factors • Prenatal: • Breach: • Normally: 2-4% • In CDH: 16% • The breach position in utero: extended knees, and flexed hips • cause dislocation of hip by ? stretch of Hamstring muscles
Etiology 3. Mechanical factors • Postnatal: • Swaddling / strapping hips adducted and extended, and knees extended المهاد – القماط – الزمام – الكوفلة
Etiology 3. Mechanical factors • Postnatal: • Swaddling / strapping hips adducted and extended, and knees extended • Proven experimentally • Proven statistically • Mechanics
Infants at risk • Positive family history: 10X • A baby girl: 4-6 X • Breach presentation: 5-10 X • Torticollis: CDH in 10-20% of cases • Foot deformities: • Calcaneo-valgus and metatarsus adductus • Knee deformities: • hyperextension and dislocation (Teratologic)
Clinical Examination • External rotation • Short one side
Clinical Examination • External rotation • Short one side • Lateralized contour • Wide perineum • In bilateral
Clinical Examination • External rotation • Short one side • Lateralized contour • Wide perineum • In bilateral • Asymmetrical folds • Anterior - posterior
Clinical Examination • External rotation • Short one side • Lateralized contour • Wide perineum • In bilateral • Asymmetrical folds • Anterior - posterior
Clinical Examination • Shortening • Might be difficult to detect early
Clinical Examination • Limitation of hip abduction in flexion
Clinical Examination • Limitation of hip abduction in flexion
Clinical Examination • Limitation of hip abduction in flexion
Clinical Examination • Special test – Hip Instability: • Ortolani / Barlow • Feel a Clunk, not hear a click!
Clinical Examination Ortolani / Barlow
Clinical Examination • Special test – Hamstring Stretch Sign: • Flex hip and knee 90o, and extend knee gradually • Normally: • feel resistance • CDH: • no resistance
Clinical Examination • After walking age: • Shortening – (if unilateral) • Limping: • Unilateral: limping • Bilateral: waddling (like a duck)
Investigation: Radiology • Early infancy: • X-ray is not reliable – all cartilage • Ultrasound is better
Radiology: X-ray • After 2-3 months: more reliable 39o 27o
Radiology: X-ray • After 2-3 months: more reliable out in
Radiology: X-ray • After 6 months: reliable • R hip out, and acetabulum open (dysplastic)
Treatment • Method depends on age • The earlier started, the easier it is • The earlier started, the better the results are • Should be detected EARLY
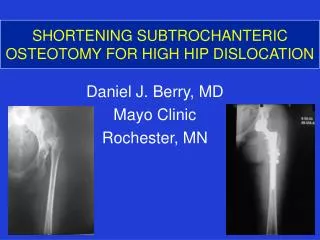
Treatment • Birth – 6m • Pavlik harness or hip spica cast • 6-12 m: • Closed reduction under GA and hip spica cast • 12 - 18 m: • Open reduction • 18 – 24 m: • Open reduction and Acetabuloplasty • 2-8 years: • Open reduction, Acetabuloplasty, and femoral shortening • Above 8 years: • Open reduction, Acetabuloplasty cutting all three pelvic bones, and femoral shortening No surgery One surgery Two surgeries Three surgeries Complex surgeries
Treatment: Neonatal • Pavlik Harness • Dynamic, effective, safe • Keeps hips abducted and flexed – for 6 weeks
Treatment: 6-12 m • Initially non-operative closed reduction UGA and immobilization in hip spica cast
Treatment: 6-12 m • Possibly closed reduction • Stable and concentric reduction • Possibly open reduction • Unstable or un-concentric reduction • Arthrography-guided
Treatment: 6-12 m • Arthrography-guided Closed Reduction Well in Dislocated Not well in
Treatment: 6-12 m Arthrography-guided Closed Reduction Acceptable Too lateralized
Treatment: 18-24 m • Open reduction – surgery • Acetabuloplasty - usually • Maybe: Femoral shortening – if high
Treatment: Above 2 years • Open reduction, and • Acetabuloplasty, and • Femoral shortening
Salter’s Acetabuloplasty Operated hip Dislocated hip
Pemberton’s Acetabuloplasty need a lot of improvement in acetabular cover
Triple Steel Acetabuloplasty • Osteotomy of: • Ilium, Pubic, • and Ischium • Rotation of • acetabulum • 12 years old, • Pain L hip • L hip not well • covered
Summary • Complex multi-factorial, endemic disease • Screening programs are needed to detect and treat cases early • Learning proper examination methods • Identify at risk groups • Efficient referral system • Proper management by specialized Drs
Summary - Infants at risk • Positive family history: 10X • A baby girl: 4-6 X • Breach presentation: 5-10 X • Torticollis • Foot deformities • Knee deformities