Download
1 / 34
350 likes | 651 Views
IAEA CODE OF PRACTICE FOR THE RADIATION STERILIZATION OF TISSUE ALLOGRAFTS. IAEA Tissue Banking Programme. Asia/Pacific region (Australia, Bangladesh, China, India, Indonesia, Japan, Korea, Malaysia Pakistan, Phillipines, Singapore, Sri Lanka, Tailand, Viet Nam )

E N D
IAEA CODE OF PRACTICEFOR THE RADIATION STERILIZATION OF TISSUE ALLOGRAFTS
IAEA Tissue Banking Programme • Asia/Pacific region (Australia, Bangladesh, China, India, Indonesia, Japan, Korea, Malaysia Pakistan, Phillipines, Singapore, Sri Lanka, Tailand, Viet Nam ) • Latin America ( Argentina, Brazil, Chile, Cuba, Mexico, peru and Uraguay) • Africa and Middle East ( Algeria, Jordan, Libya, Zambia, Iraq) • Europe ( Greece, Poland, Turkey, Slovakia )
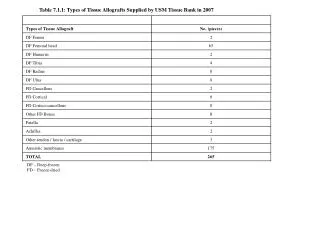
Graft production 1988-2000 • Cancellous bone 69195 • Massive bone allografts 8588 • Skin, Amnion 96645 • Other 50278 Other- dura mater, demineralised bone, xenografts, pericardium, tendon, ligaments, fascia
The IAEA Programme International Standards for Tissue Banks Code of Practice for the Radiation Sterilisation of Tissues Handbook for Public and Professional Awareness Internet Training
Development of a Code of Practice • Why do we need a Code of Practice ? • Existing ISOs and TR for health products • ISO 11137 ( methods 1 and 2 ) • ISO TR 13409 ( small batch size ) • ISO 15844 ( single batch )
ISO 11137 Dose setting methods Overview of method • Inactivation of microbial population • Probability model • Bioburden due to mix of microbial species each with a unique D10 value • Probability of sterility defined in terms of initial number of organisms and their D10 values • Products (or portions) are tested for sterility for doses lower than the sterilisation dose
ISO 11137 Dose setting methods Method 1 Dose setting - bioburden method • Depends on greater response to radiation of product microflora than ‘reference microflora’ • Average bioburden determined (for whole product unit or Sample Item Portion (SIP)) • Dose for SAL 10-2 selected for verification dose • Samples irradiated at verification dose and tested for sterility (one or two positives in 100 samples) • If valid, dose determined for SAL of 10-6
ISO 11137- Dose setting methods Method 2 - Dose setting using fraction positive information from incremental doses to determine extrapolation factor Radiation resistance of microflora on product is determined using incremental doses to establish dose for SAL of 10-2 Validity depends on response ofmicroflora to extrapolated doses Two approaches - 2A ‘normal’ bioburden - 2B for products with low, consistent bioburden
ISO/TR 13409 Technical Report This Technical Report is an adaptation of methods 1 in ISO 11137 and allows the use of as little as 10 samples to determine the averagebioburden. Again a statistical approach is used which means that an upper limit of SAL 10-1 (for product unit) is used for the determination of the verification dose. - increased probability of failing the verification dose experiment, particular for product sampleswith low bioburden (less than1cfu/unit) -used tosubstantiate 25kGy as an appropriate dose to achieve an SAL of 10-6.
Development of an International Standard Q - Can the existing standards for the sterilisation of medical products be used or modified for tissues? Major issues are: • No standard tissue allografts in terms of bioburden,shape, size,materials and therefore statistical approaches to establish verification doses or a routine basis are more difficult • Sterilisation of viruses in addition to bacterial contamination. May require unacceptably high doses for SAL of 10-6 • Sampling issues with irregular shaped and non-homogeneous tissues • Absorbed dose determinations - irregular size of sample and, in some cases, wide range of density
Inactivation of viruses in tissues VirusD10 (kGy)Dose (6 log) BVDV <3.0 18.0 PRV 5.29 31.7 HAV 5.31 31.9 HIV-2 7.09 42.5 PV-1 7.13 42.8 3PV 7.27 43.6 * Pruss, Kao, Gohs, Moenig, von Versen and Pauli
Tissue allografts v health products, issues • uniformity of samples- size and density • viral contamination • low numbers in sample
Validation of the processes • Pre-sterilisation • Sterilisation
Pre-sterilisation processes • Qualification of Tissue Bank facilities • Qualification of the tissue donors • Qualification of tissue processing and preservation
Qualification of the tissue bank • Laboratories for reception,preservation and storage ( Standards document ) • Laboratories for microbiology
Qualification of the tissue donors • Aim : to procure tissues free of transmissible disease
Qualification of the tissue donors • Time of retrieval • Age of donor • Medical, social and sexual history of donor • Physical examination • Serological tests • Autopsy
Qualification of processing and preservation- tissue allografts • bone, cartilage • ligaments, fascia • tendons, dura mater • skin, amnion
Qualification of processing and preservation- processing • Removal of bone marrow • De-fatting • Pasteurisation • Antibiotic treatment • Percolation • Hypochlorite, ethyl alcohol, glycerol
Qualification of processing and preservation • Choice of process influenced by : • preferred practice of Bank • nature of tissue • degree of contamination
Qualification of processing and preservation • Preservation may include: • freeze drying, deep freezing • air and heat drying • chemical treatments
Qualification of processing and preservation • Aim : to produce tissues • less than 1000 cfu per allograft to allow a 25 kGy dose ( or less ) to achieve an SAL of 10-6
Processing and preservation-maintenance of validation • Audit of procured tissue ( origin, history, testing ) • Audit of labs. • Audit of bioburden of samples prior to and after processing and preservation • Audit of methodology ( ability to reduce bioburden )
Process specification • Tissue allograft types covered • Tissue selection parameters • Detailed methodology • Details of equipment, labs., etc • Details of routine maintenance • Details of documentation
Validation of sterilisation process • Qualification of tissue allografts and packaging • Qualification of irradiation facility • Process qualification
Qualification of allografts for sterilisation • Number , type and resistances of organisms • Sample Item Portion to determine bioburden • Use SDR if no knowledge of bioburden distribution
Selection of dose setting method • For small sample sizes and assuming SDR • adapt Method 1 of ISO 11137 • use ISO TR 13409 for 25 kGy
Selection of dose setting method • For known distributions, ( ie not SDR ), use appropriate survival equation
Selection of dose setting method for 25 kGy • Use ISO TR 13409 • Use AAMI TIR 27 : 2001
Determination of sterilisation dose ( AAMI TIR 27 ) • Essentially uses an artificial survival curve more resistant than SDR • therefore predicts verification doses which are higher and less likely to fail
Worked examples • Amnion, low sample numbers and low resistance • Dose for SAL 10-6 is 14 kGy
Worked example • Amnion, 25 kGy dose needed only • VD from ISO 13409 failed • VD from AAMI 27 passed
Worked example • Bone samples , SDR, 25 kGy • ISO TR 13409 used successfully