Download
1 / 17
170 likes | 468 Views
Urgent pleural disorders Aleš Rozman University Clinic of Respiratory Diseases and Allergy, GOLNIK, Slovenia Portorož – 8th May 2009. Pleural emergencies: haemorrhage - haemothorax elevated pleural pressure - tension pneumothorax - massive pleural effusion. 1. Haemothorax.

E N D
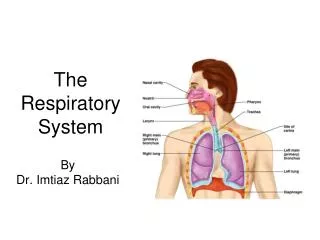
Urgent pleural disorders Aleš Rozman University Clinic of Respiratory Diseases and Allergy, GOLNIK, Slovenia Portorož – 8th May 2009
Pleural emergencies: • haemorrhage • - haemothorax • elevated pleural pressure • - tension pneumothorax • - massive pleural effusion
1. Haemothorax = pleural fluid with Ht > 50% blood Ht • CAUSES: • chest trauma: penetrating / non – penetrating • (lung blood vessels, chest wall, diaphragm, pleural adhesions, mediastinum, large vessels, abdomen) • iatrogenic • (pleural biopsy, subclavian or jugular CVC placement, thoracentesis, transthoracic or transbronchial NA, esophageal variceal TH,...) • nonthraumatic • (pleural malignancy, anticoagulant TH, spontaneous rupture of vessel (AO aneurism), bleeding disorder, thoracic endometriosis,...)
1. Haemothorax • DG: • CXR • chest CT – for all patients with severe chest trauma • thoracentesis transudate haemothorax with higher attenuation (> 35 HU)
1. Haemothorax • TH: • immediate tube thoracostomy • evacuation of blood • stop bleeding by apposition of pleural surfaces • evaluation of blood loss • may decrease incidence of empiema or fibrothorax • autotransfusion possible • thoracotomy (cca 15%) • immediate drainage of > 20 ml/kg of blood • persistent bleeding > 200 ml/h • cardiac tamponade, vascular injury, pleural contamination, major air leaks,... • TH of shock, blood and fluid replacement,...
1. Haemothorax • Complications: • retention of clotted blood (evacuation if > 30% of hemiTHX) • empyema (3 – 5%) • – shock, contamination, prolongued drainage, abdominal injuries • exudative pleural effusion (15 – 30%) • fibrothorax (< 1%)
2. Tension PTHX = air in the pleural space, which pressure exceeds the atmospheric pressure throughout expiration (inspiration). • CAUSES – any type of PTHX: • with mechanical ventilation / NIPPV • during cardiopulmonary resuscitation • in divers • in air travel • in spontaneously breathing person at constant pressures (airway, environment) • improper chest tube handling
Pneumoscrotum secondary to bilateral tension pneumothorax Di Capua-Sacoto C, Bahilo-Mateu P, Ramírez-Backhaus M, Gimeno-Argente V, Pontones-Moreno JL, Jiménez-Cruz JF Servicio de Urología. Hospital Universitario La Fe. Valencia. Spain Actas Urol Esp. 2008;32(7):756-758 ABSTRACT PNEUMOSCROTUM SECONDARY TO BILATERAL TENSION PNEUMOTHORAX We report a case of pneumoscrotum secondary to a large bilateral tension pneumothorax. Although pneumoscrotum is an infrequent clinical condition that is generally resolved by means of conservative management, it may be a symptom of a serious and potentially life-threatening process. The management of pneumoscrotum should be directed to resolve the underlying cause. Key words: Pneumoscrotum. Pneumothorax. Complications.
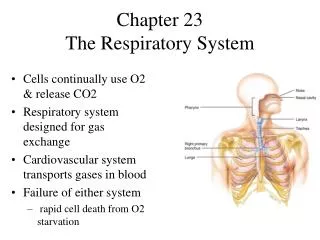
2. Tension PTHX • Patophysiology: • impaired venous return and decreased cardiac output • V/Q mismatch - profound hypoxia • Clinical manifestations: • sudden deterioration • dyspnoe, cyanosis, tachicardia, profuse sweating • hypotension, low O2 saturation, distended neck veins • subcutaneous emphysema, unilateral hyperinflation • respiratory acidosis, hypoxemia • sudden increse in plateau and peak pressures (volume – type vent.) • sudden drop of tidal volumes (pressure – type vent.)
2. Tension PTHX mediastinal shift hyperinflation collapsed lung low hemidiaphragm
2. Tension PTHX • TH: • medical emergency – clinical diagnosis • do not wait for CXR • 100% O2 • observation, auscultation, percussion • needle & syringe with saline – 2nd anterior ICS • bubbles? – replace with large - bore needle • prepare for tube thoracostomy
3. Massive pleural effusion • CAUSES: • malignant pleural effusion • PATOPHYSIOLOGY: • impaired venous return and decreased cardiac output • V/Q mismatch - profound hypoxia
3. Massive pleural effusion • Clinical manifestations: • gradual deterioration • dyspnoe, cyanosis, tachicardia • hypotension, low O2 saturation, distended neck veins • unilateral distension of THX, absent respiratory mobility
3. Massive pleural effusion mediastinal shift distension
3. Massive pleural effusion • TH: • thoracentesis for symptomatic relief (500 – 1000 ml) • consider chest tube and pleurodesis • avoid rapid evacuation of all pleural fluid (reexpansion lung edema, PTHX)
3. Conclusions • Haemothorax and tension pneumothorax can be iatrogenic. • Careful monitoring of patients and early recognition of complications should be a standard after each invasive procedure.
University Clinic Golnik, Slovenia Thank you.