Download

1 / 18
280 likes | 989 Views
Osteoporosis. Dr. Lauren Phillips Sugar Land Women’s Health. Osteoporosis- What is it?. A common disorder resulting in low bone mass, skeletal fragility, and an increased risk of fracture 15% of women over 50 have osteoporosis 1.3 million fractures per year in the US. Bone Remodeling.

E N D
Osteoporosis Dr. Lauren Phillips Sugar Land Women’s Health
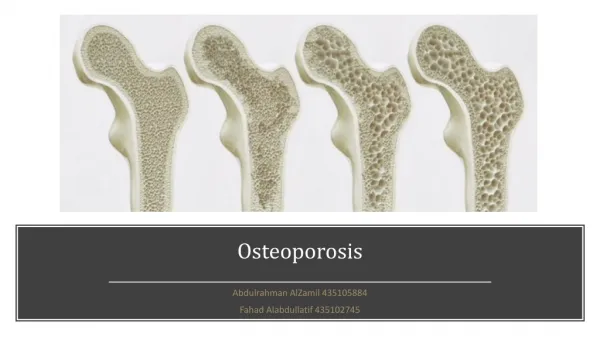
Osteoporosis- What is it? • A common disorder resulting in low bone mass, skeletal fragility, and an increased risk of fracture • 15% of women over 50 have osteoporosis • 1.3 million fractures per year in the US
Bone Remodeling • Osteoblasts- bone forming cells • Osteoclasts- bone destroying cells • These cells must cooperate to maintain adequate bone metabolism • Regulated by calcium, vitamin D, estrogen, calcitonin, PTH, and inflammatory markers called cytokines
Who is at risk? • Postmenopausal women • Previous fracture • Long-term steroid therapy • Low body weight (less than 58 kg [127 lb]) • Family history • Cigarette smoking • Excess alcohol intake • Premature or surgical menopause, malabsorption, chronic liver disease, inflammatory bowel disease • Caucasian or Asian ethnicity
Screening for osteoporosis • Bone density testing: Dual energy x ray absorpiometry (DXA)- most useful and reliable test for measuring BMD (bone mineral density). It’s a special type of x ray that gives off little radiation.
Who should get screened? • All women age greater than 65 • Postmenopausal women with one or more risk factors • No consensus regarding frequency of screening; most practitioners make individual recommendations for patients based on age and risk factors • Typically every 2-5 years after menopause or yearly if severely osteopenic or osteoporotic
Measuring bone mineral density • T score: the standard deviation (SD) difference between a patient's BMD and that of a young-adult reference population • Z score: a comparison of the patient's BMD to an age-matched population (less than -2.0 is abnormal)
Diagnosing osteopenia and osteoporosis • Measure T scores at spine and hip • T score values: • +1 to -1: normal bone density • -1 to -2.5: osteopenia • -2.5 and lower: osteoporosis
Treatment • All postmenopausal women with a history of vertebral or hip fracture • Women with a T score of less than -2.5 (osteoporosis) • T-score between -1.0 and -2.5 (osteopenia) with high risk of fracture such as glucocorticoid use or total immobilization. • Osteopenia plus a 10-year probability of hip fracture ≥3 % or a 10-year probability of any major osteoporosis-related fracture ≥20% based upon the WHO algorithm. • www.shef.ac.uk/FRAX
Non pharmacologic treatment • Calcium and vitamin D intake: 1200 mg/ day calcium and 800 mg vit D per day • Exercise: weight bearing exercise for at least 30 min 3 times a week. • Smoking cessation
Non Pharmacalogic Therapy • Osteostrong.me- a wellness center uses a BioDensity device to build bone mass and promote muscle growth • Weekly visits with improvement each week • 4-7% increase in BMD after 12 months
Pharmacologic therapy • Bisphosphates: Fosamax, Actonel (taken weekly) Boniva (taken monthly), Reclast (IV once yearly) • Causes osteclasts to undergo apoptosis (cell death) • First line therapy- can use safely 5-10 years • Must take on empty stomach and stay sitting up for 30 min • Side effects typically mild and include GI upset, flu like symptoms • Osteonecrosis of jaw approx 1/10,000
Pharmacolgic therapy • Raloxifene (Evista): a selective estrogen receptor modulator. • Increases estrogen absorption in the spine but not other organs. Also decreases risk of breast cancer and LDL cholesterol, but increases risk of DVT slightly • Not as efficatious as bisphosphonates or HRT. • May increase hot flashes
Pharmacologic Therapy • HRT- estrogen alone or estrogen plus progesterone • Effective • Due to WHI study in 2002, no longer used solely for the prevention or treatment of osteoporosis. Exceptions include women with persistent menopausal symptoms and those who cannot tolerate the other drugs.
Pharmacologic Therapy • Prolia- stops the production of osteoclasts • Injection twice a year • Not first line • Side effects related to injection, hypocalcemia, infections • Not for people who have hypocalcemia, malabsorption, kidney problems, have had thyroid or parathyroid surgery
Goals of Therapy • Introduce/ continue healthy lifestyle habits • Prevent fractures! • Slow or stop progression of bone loss • Improve T scores • Re-evaluate every 1-2 years
Contact information Dr. Lauren Phillips 17510 West Grand Parkway South Suite 430 Sugar Land, TX 77479 713-578-3823 www.obgynassociates.com www.mysugarlandobyn.com