Download
1 / 47
520 likes | 616 Views
Bundle Branch Blocks and Hemiblocks. Take Home Points. Bundle branch blocks are best characterized on ECG by: prolongation of the QRS > 0.12 sec Region of slowed conduction determines the orientation of the terminal QRS vector and localizes the block

E N D
Take Home Points • Bundle branch blocks are best characterized on ECG by: • prolongation of the QRS > 0.12 sec • Region of slowed conduction determines the orientation of the terminal QRS vector and localizes the block • Hemiblocks do not typically show QRS prolongation, rather they reveal axis deviation corresponding to the QRS terminal vector • Ventricular conduction blocks are common and can represent a spectrum from normal variant to serious pathology
Normal Anatomy of the Cardiac Conduction System • SA Node • AV Node • Bundle of His • Left and R Bundle Branches • Septal Fascicle • LAF • LPF • Purkinje fibers • Myocardium www.nottingham.ac.uk/.../cardiac_conduction.gif
Anatomy of the Ventricular His-purkinje Conduction System Left bundle branch Right bundle branch Left anterior fascicle Septal fascicle Left posterior fascicle
Bundle Branch Blocks • Intrinsic impairment of conduction in the left or right bundle branches • Can be chronic or intermittent • Can be rate dependant • Can be present without cardiac disease • Most often due to CAD or HTN causing ischemic or degenerative changes
EKG Manifestations of BBBs • Widened QRS complex > 0.12 sec • Results from slow myocyte-to-myocyte conduction causing prolonged ventricular depolarization • incomplete (0.8-0.11s) or complete (>0.12s) • Terminal QRS is sluggish and reflects the electric forces in the affected ventricle. • LBBB = terminal QRS is superior, posterior, and left • RBBB = terminal QRS in inferior, anterior, and right • Repolarization abnormalities • ST and T-wave oriented opposite of the terminal QRS
Right Bundle Branch Block Left bundle branch Right bundle branch Left anterior fascicle Septal fascicle Left posterior fascicle
Phase 1: Initial QRS in RBBB • The initial QRS deflection represents the septum depolarizing from left to right. This conduction is mediated by the septal fascicle arising from the left bundle branch • The initial QRS is unchanged in RBBB because conduction is independent of the right bundle branch
Phase Two: RBBB • Following the initial QRS, the left ventricle rapidly depolarizes via conduction from the LAF and LPF. • The right ventricle is delayed. • This produces a QRS vector oriented to the left and posterior. • The left ventricle is normally dominant during the QRS and thus the EKG still shows no abnormally
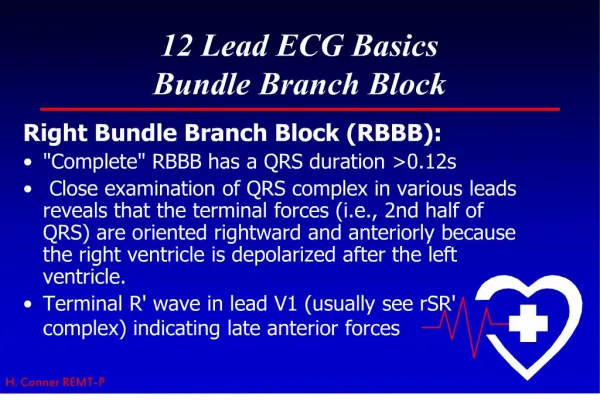
Phase 3: Terminal QRS in RBBB • Following left ventricular depolarization, there continues to be delayed depolarization of the right ventricle via slow myocyte-to-myocyte spread. • The right ventricle is now the dominate electrical force and therefore the terminal QRS vector is oriented to the right and anterior. This shows on an ECG as an additional tall upright R’ wave in V1 and a deep S wave in V6.
RBBB • Initial QRS remains normal • Middle portion of QRS remains normal • Terminal QRS is sluggish and dominated by right ventricular forces
Right Bundle Branch Block Notice the wide RSR' complex in lead V1 and the QRS complex in lead V6. Inverted T waves in the right precordial leads (in this case V1 to V3) are common with right bundle branch block and are called secondary T wave inversions.
RBBB RBBB
RBBB • Incidence increases with age • Can occur as a normal variant • Most common cause is CAD (LAD) • Other causes include both structural and functional causes • Structural: anything causing RV dilatation or hypertrophy, (acute PE, cor pulmonale, DCM, ect), trauma (right heart cath, steering wheel, CABG, ablation) • Functional: rate-related bundle branch block
Differential Diagnosis of RBBB • Myocardial infarction • Pulmonary embolism • Chronic obstructive lung disease/cor pulmonale • Pulmonary hypertension (primary or secondary) • Hypertensive heart disease • Degenerative disease of the conduction system • Brugada syndrome • Arrhythmogenic RV dysplasia • Cardiomyopathy • Chagas disease • Congenital heart disease (eg, Ebstein anomaly)
RBBB: prognosis and treatment • Prognosis depends on underlying etiology • Worse prognosis for patients with type II second degree atrioventricular (AV) block or multifascicular block • Generally good prognosis for patients without underlying heart disease • NO treatment necessary for isolated asymptomatic RBBB • Pacing may be necessary for symptomatic patients or those with other AV or multifascicular block
RBBB and MI • T-wave inversions may be seen in leads V1-V3, II, III, and aVF secondary to the additional rSR’-type complex (changes to QRS axis) • ST and T wave changes in the same direction as the terminal QRS complex should be considered primary abnormalities (ventricular gradient not between 0º and 90º in the frontal plane) • Since RBBB does not alter initial phase of ventricular depolarization, RBBB does not mask abnormal Q waves seen in MI
Left Bundle Branch Block Left bundle branch Right bundle branch Left anterior fascicle Septal fascicle Left posterior fascicle
Phase one: Initial QRS in LBBB • Normally the LBB begins the initial QRS with left-to-right septal depolarization • In LBBB the first phase is altered. The initial QRS vector remains slightly anterior and oriented right-to-left.
Phase two: LBBB • The right ventricle is stimulated first via the intact RBB while the left ventricle proceeds by slow slow cell-to-cell depolarization • The RV is not seen on ECG since it is overwhelmed by larger forces from the LV • This slow depolarization through the LV creates a widened QRS complex with upward deflexions in the lateral leads. • In LBBB all phases of ventricular depolarization are effected
LBBB • Initial QRS orientation is right-to-left • Middle and terminal QRS forces are dominated by the larger left ventricular forces • Slow conduction causes long QRS deflection
LBBB and MI • T-waves in leads with tall R waves (left precordial leads) are inverted secondary to changes in QRS in LBBB • T-wave inversions in the right precordial leads cannot be explained by LBBB • MI can be difficult to diagnose on ECG in LBBB because Q waves/ ST elevations can be masked • Exercise stress testing is of limited value in CAD • The 2002 American College of Cardiology/American Heart Association (ACC/AHA) guidelines concluded that there is no level of ST segment depression that confers diagnostic significance during exercise ECG testing in patients with LBBB • Can use myocardial perfusion imaging (MPI)
LBBB • Incidence increases with age • Almost always associated with underlying heart disease • Most common causes include CAD, HTN, dilated CM (hypertrophy/dilatation of LV) • Other causes include valvular diseases-rheumatic heart disease, aortic stenosis, ect • Rarely results from primary degeneration of the conduction system • Rate- or acceleration-dependent LBBB
LBBB prognosis and treatment • Also depends on underlying cardiac conditions • Worse prognosis for patients with type II second degree atrioventricular (AV) block or multifascicular block • Prognosis depends on age- worse with increasing age • Isolated LBBB is more likely than RBBB to progress to high-degree AV block and has worse mortality • NO treatment for asymptomatic isolated LBBB is necessary • Pacing may be necessary for symptomatic patients or those with other AV or multifascicular block
Hemiblock / Fascicular Block LBB • The Left Bundle Branch divides into 3 separate fascicles • Septal fascicle innervates the ventricular septum • The anterior fascicle runs toward the anteriolateral papillary muscle and projects anterior, leftward, and superior • The posterior fascicle runs toward the posterior papillary muscle and projects posterior, rightward, and inferiorly • Normal electrical activation of the LV spreads simultaneously from the base of the two papillary muscles RBB LAF SF LPF
Hemiblock / Fascicular block cont. • A fascicular block occurs when you have impaired conduction down one division of the LBB • The block is manifested on EKG as QRS axis deviation • No / minimal QRS prolongation (0.09 – 0.11 sec) • Most commonly due to CAD and MI; also cardiomyopathies
Left Anterior Fascicular Block LBB • With LAFB the LPF carries the initial depolarization inferior, posterior and to the right • Then the vector shifts unopposed to the left, anterior, and superior • Common cause of left axis deviation RBB LAF LPF
LAFB: ECG findings • QRS duration < 0.1 sec • Left axis deviation (Usually -45° to -90°) • No other identified cause of left axis deviation • Tall R waves in I and aVL • Big S waves in II, III, and aVF
LAFB QRS has normal duration Left axis deviation
LAFB QRS has normal duration Left axis deviation Tall R waves in I and aVL Deep S waves in II, III, and aVF http://askdrwiki.com/mediawiki/images/thumb/c/cd/LAFB.jpg/750px-LAFB.jpg
Left Posterior Fascicular Block LBB • With LPFB the LAF carries the depolarization left, anterior and superior • THEN the vector shifts unopposed inferior, posterior, and to the right • Rare cause of right axis deviation • LPFB is less likely to be caused by ischemia because it receives dual blood supply from RCA and LAD RBB LAF LPF
LPFB: ECG findings • Normal duration of QRS < 0.1 sec • Right axis deviation (+90° to +180°) • No other identified cause of right axis deviation • Big S waves in I and aVL • Big R waves in II, III, and aVF
Bifascicular blocks: RBBB and LAFB • QRS > 0.12s • RSR’ in V1 • Wide and slurred S waves in I, V5, V6 • First half (0.06s) of QRS having frontal plane axis of -30° to -90° • Initial R wave in inferior leads
Bifascicular blocks: RBBB and LPFB • QRS>0.12s • RSR’ in V1with R’ broad and slurred • Wide and slurred S waves in I, V5, V6 • First half (0.06s) of QRS having frontal plane axis of +90° or further to the right with rS deflection in lead I and qR waves in II, III, and aVF
Unknown? QRS prolonged > 0.12 sec Terminal forces are left and posterior Dx: LBBB http://sinaiem.org/wp-content/uploads/2007/07/lbbb_ekg1.jpg
Unknown? QRS Prolongation > 0.12 sec RSR’ in V1, V2 ST, T-wave abnormalities Slurred terminal S wave in I, V3, V4, V5, V6 Dx: RBBB www.sbhemresidency.com/assets/images/EKG_2-13
Unknown? QRS has normal duration Right axis deviation Dx: LAFB
Unknown? QRS Prolongation > 0.12 sec RSR’ in V1, V2, V3 ST, T-wave abnormalities Slurred terminal S wave in I, aVL, V4, V5, V6 Dx: RBBB askdrwiki.com/mediawiki/images/b/bb/RBBB.PNG
Unknown? QRS prolonged > 0.12 sec Terminal forces are left and posterior Dx: LBBB http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=cardio&part=A39
Unknown? QRS has normal duration Left axis deviation Dx: LAFB http://askdrwiki.com/mediawiki/images/thumb/c/cd/LAFB.jpg/750px-LAFB.jpg
Take Home Points • Bundle branch blocks are best characterized on ECG by: • prolongation of the QRS > 0.12 sec • Region of slowed conduction determines the orientation of the terminal QRS vector and localizes the block • Hemiblocks do not typically show QRS prolongation, rather they reveal axis deviation corresponding to the QRS terminal vector • Ventricular conduction blocks are common and can represent a spectrum from normal variant to serious pathology