Download
1 / 1
10 likes | 224 Views
An Audit of breast radiotherapy reproducibility and an assessment of the role of breast volume on field placement accuracy. . Heidi Probst PhD , Sarah Hielscher BSc ( Hons ), Janet Johnson MSc, Amy Taylor BSc ( Hons )

E N D
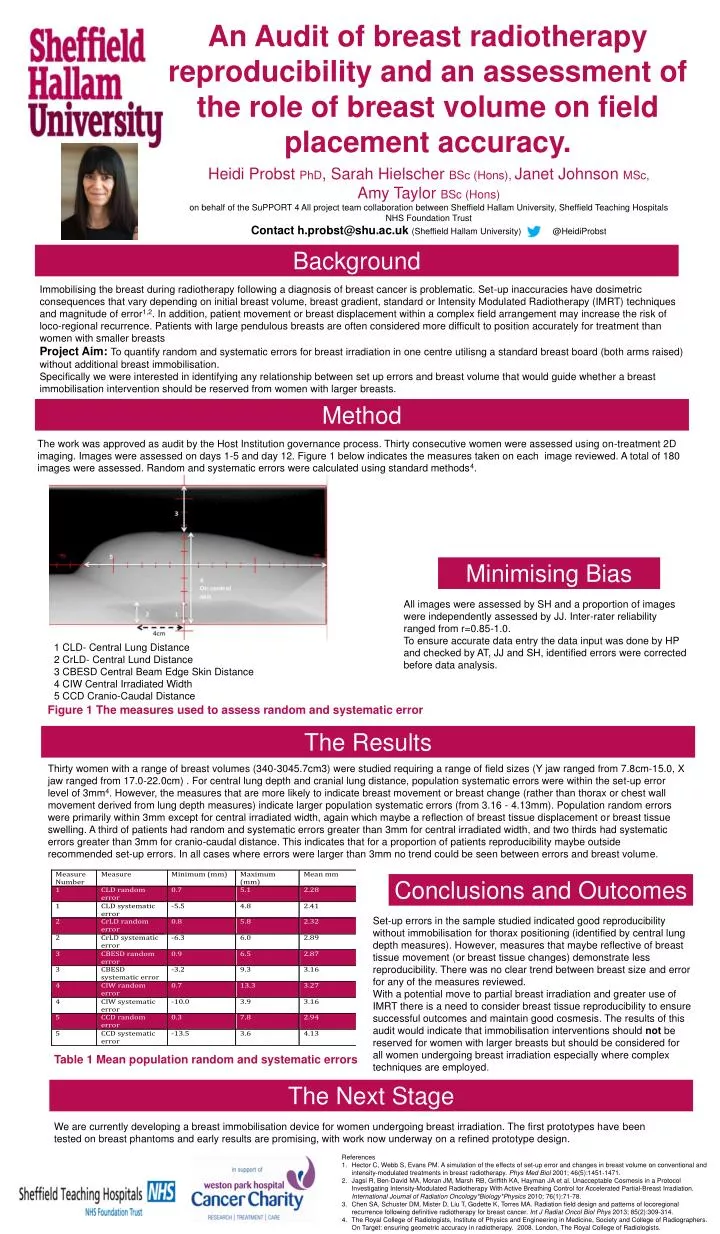
An Audit of breast radiotherapy reproducibility and an assessment of the role of breast volume on field placement accuracy. Heidi Probst PhD, Sarah HielscherBSc (Hons), Janet Johnson MSc, Amy Taylor BSc (Hons) on behalf of the SuPPORT 4 All project team collaboration between Sheffield Hallam University, Sheffield Teaching Hospitals NHS Foundation Trust Contact h.probst@shu.ac.uk (Sheffield Hallam University) @HeidiProbst Background Immobilising the breast during radiotherapy following a diagnosis of breast cancer is problematic. Set-up inaccuracies have dosimetric consequences that vary depending on initial breast volume, breast gradient, standard or Intensity Modulated Radiotherapy (IMRT) techniques and magnitude of error1,2. In addition, patient movement or breast displacement within a complex field arrangement may increase the risk of loco-regional recurrence. Patients with large pendulous breasts are often considered more difficult to position accurately for treatment than women with smaller breasts Project Aim: To quantify random and systematic errors for breast irradiation in one centreutilisng a standard breast board (both arms raised) without additional breast immobilisation. Specifically we were interested in identifying any relationship between set up errors and breast volume that would guide whether a breast immobilisation intervention should be reserved from women with larger breasts. Method The work was approved as audit by the Host Institution governance process. Thirty consecutive women were assessed using on-treatment 2D imaging. Images were assessed on days 1-5 and day 12. Figure 1 below indicates the measures taken on each image reviewed. A total of 180 images were assessed. Random and systematic errors were calculated using standard methods4. Minimising Bias All images were assessed by SH and a proportion of images were independently assessed by JJ. Inter-rater reliability ranged from r=0.85-1.0. To ensure accurate data entry the data input was done by HP and checked by AT, JJ and SH, identified errors were corrected before data analysis. 1 CLD- Central Lung Distance 2 CrLD- Central Lund Distance 3 CBESD Central Beam Edge Skin Distance 4 CIW Central Irradiated Width 5 CCD Cranio-Caudal Distance Figure 1 The measures used to assess random and systematic error The Results Thirty women with a range of breast volumes (340-3045.7cm3) were studied requiring a range of field sizes (Y jaw ranged from 7.8cm-15.0, X jaw ranged from 17.0-22.0cm) . For central lung depth and cranial lung distance, population systematic errors were within the set-up error level of 3mm4. However, the measures that are more likely to indicate breast movement or breast change (rather than thorax or chest wall movement derived from lung depth measures) indicate larger population systematic errors (from 3.16 - 4.13mm). Population random errors were primarily within 3mm except for central irradiated width, again which maybe a reflection of breast tissue displacement or breast tissue swelling. A third of patients had random and systematic errors greater than 3mm for central irradiated width, and two thirds had systematic errors greater than 3mm for cranio-caudal distance. This indicates that for a proportion of patients reproducibility maybe outside recommended set-up errors. In all cases where errors were larger than 3mm no trend could be seen between errors and breast volume. Conclusions and Outcomes Set-up errors in the sample studied indicated good reproducibility without immobilisation for thorax positioning (identified by central lung depth measures). However, measures that maybe reflective of breast tissue movement (or breast tissue changes) demonstrate less reproducibility. There was no clear trend between breast size and error for any of the measures reviewed. With a potential move to partial breast irradiation and greater use of IMRT there is a need to consider breast tissue reproducibility to ensure successful outcomes and maintain good cosmesis. The results of this audit would indicate that immobilisation interventions should not be reserved for women with larger breasts but should be considered for all women undergoing breast irradiation especially where complex techniques are employed. Table 1 Mean population random and systematic errors The Next Stage We are currently developing a breast immobilisation device for women undergoing breast irradiation. The first prototypes have been tested on breast phantoms and early results are promising, with work now underway on a refined prototype design. • References • Hector C, Webb S, Evans PM. A simulation of the effects of set-up error and changes in breast volume on conventional and intensity-modulated treatments in breast radiotherapy. PhysMedBiol 2001; 46(5):1451-1471. • JagsiR, Ben-David MA, Moran JM, Marsh RB, Griffith KA, Hayman JA et al. Unacceptable Cosmesis in a Protocol Investigating Intensity-Modulated Radiotherapy With Active Breathing Control for Accelerated Partial-Breast Irradiation. International Journal of Radiation Oncology*Biology*Physics 2010; 76(1):71-78. • Chen SA, Schuster DM, Mister D, Liu T, Godette K, Torres MA. Radiation field design and patterns of locoregional recurrence following definitive radiotherapy for breast cancer. Int J RadiatOncolBiolPhys 2013; 85(2):309-314. • The Royal College of Radiologists, Institute of Physics and Engineering in Medicine, Society and College of Radiographers. On Target: ensuring geometric accuracy in radiotherapy. 2008. London, The Royal College of Radiologists.