Download
1 / 49
500 likes | 862 Views
Abdominal Wall Function: The Unstudied Aspect of Ventral Hernia Repair . Drew Reynolds, M.D. Surgery Grand Rounds University of Kentucky January 25, 2012. Objectives:. Briefly Review the Anatomy & Physiology of the abdominal wall. Explore the impact of a hernia on abdominal wall function.

E N D
Abdominal Wall Function: The Unstudied Aspect of Ventral Hernia Repair Drew Reynolds, M.D. Surgery Grand Rounds University of Kentucky January 25, 2012
Objectives: Briefly Review the Anatomy & Physiology of the abdominal wall. Explore the impact of a hernia on abdominal wall function. Discuss the relevance of abdominal wall function in the care of hernias. Discuss the modalities proposed to assess abdominal wall function. Future directions.
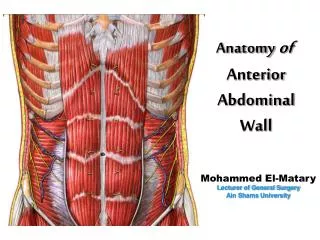
Anatomy External Oblique: Origin: post. aspect lower 8 ribs (Serratus Ant./Latissimus) Insertion: Iliac Crest, inguinal ligament, ant. Rectus sheath, linea alba Internal Oblique: Origin: Iliac fascia/crest Insertion: lower 3-4 ribs, Rectus sheath, linea alba, cremasters. TransversusAbdominis: Origin: Iliac fascia/crest, inguinal ligament, lower ribs (Diaphragm) Insertion: Rectus sheath, linea alba, conjoint tendon
Anatomy Rectus Abdominis: Origin: 5th-7th costal cartilages Insertion: pubic symphysis/crest Innervation (ALL): T7-T12, L1-2 Ventral Rami; run between internal and transversus, pierce lateral rectus sheath Blood Supply: Lateral muscles: lower intercostalaa., Deep Circumflex Iliac a., lumbar aa. Rectus: Sup./Inf. Epigastricaa.; intercostalaa.
Function External Oblique: Trunk rotation; lateral spine flexion; upright spine stabilization; Valsalva Internal Oblique: Trunk rotation; lateral spine flexion; Trunk flexion; Valsalva TransversusAbdominis: Upright spine stabilization; Valsalva Rectus Abdominis: Trunk flexion; Trunk rotation; Valsalva Compression and containment of the abdominal viscera. Contributing to the support and movement of the trunk, spine, and pelvis.
Lots of Questions!!! What does the presence of a hernia do to the function of the abdominal wall muscles? If you fix the hernia, does function improve, or is irreversible damage done? Do hernia-induced changes in function of the abdominal wall muscles contribute to hernia recurrence? Do certain types of hernia repair offer long-term functional advantages over another? Are there prophylactic measures that we should be undertaking after routine laparotomy to prevent incisional hernia formation?
Incidence of Incisional Hernia 337 patients completed 10 years of follow-up. Single examiner. 11% Incidence of incisional hernia. 35% of recurrences appeared at 5 years or later. 374 patients 20% Incidence of Incisional hernia at 12 months (292 pts.) 142 patients at 8 years – 5 incisional hernias.
Incidence 11-20% Incidence of Incisional hernia. You do the math. 4-5 Million Laparotomies Annually in the U.S. 440,000 Incisional Hernias generated/year!!!
Mesh!! Repair and Recurrence NEJM, 2000. Annals of Surgery, 2004
LuijendijkNEJM, 2000 Independent Risk factors for Recurrence: Suture Repair Prostatism (men) History of Infection History of Surgery for AAA Size of defect did not affect recurrence rate!
Burger, Luijendijk, et al. Annals of Surgery, 2004 126 patients completed Follow-Up. 25 New Recurrences were discovered. 63% vs. 32%
Burger, Luijendijk, et al. Annals of Surgery, 2004 Recurrence continues up to 10 years after incisional hernia repair! 10-year Cumulative Recurrence rate of 63% is an unacceptable number. 32% recurrence rate for mesh repair still isn’t great! “Suture Repair of Incisional hernia should be abandoned.”
Washington State Hospital Discharge Database 10,822 patients Incisional hernia repair; 1987-1999 12.3% underwent at least one reoperative repair within 5 first years after initial repair. (23.1% within 13 yrs) 5 year reoperative rates: 23.8% after 1st reoperation 35.3% after 2nd reoperation 38.7% after 3rd reoperation
Flum, et al.Annals of Surgery, 2003 Mesh use increased from 34.2% in 1987 to 65.5% in 1999. The rate of reoperation over time was significantly higher for non-mesh operations.
Flum, et al.Annals of Surgery, 2003 Conclusions: “Incisional hernia repair is associated with high cumulative rates of reoperative repairs.”
Risk Factors for Hernia: Infection, Obesity, Smoking, etc. Individual Tissue Biology: Extracellular Matrix Components Collagen MMPs Aortic Aneurysms; Marfan’s; Ehlers-Danlos; OsteogenesisImperfecta
Collagen I/III Ratios: Incisional Hernia patients – 1.0 Normal Controls – 2.1 (p <0.01) Type I Collagen – thick fibers/high tensile strength Type III Collagen – thin bundles A decreased ratio of Type I/III corresponds to less tissue stability.
Abdominal Wall Function What is lost with a hernia?
Rat Incisional Hernia Model 3 groups: Uninjured - normal Sham – healed laparotomy Hernia 35 DAYS
Dubay and Franz, et al.Annals of Surgery, 2007 Incisional Hernia Model: Internal Oblique Muscle
Dubay and Franz, et al.Annals of Surgery, 2007 Incisional Hernia Model: Internal Oblique Muscle Uninjured Sham (Healed) Hernia
Dubay and Franz, et al.Annals of Surgery, 2007 Incisional Hernia Model: Internal Oblique Muscle – Collagen Deposition Uninjured Sham (Healed) Hernia
Dubay and Franz, et al.Annals of Surgery, 2007 What does this mean? Abdominal wall musculature – Dynamic Equilibrium of Load Forces Laparotomy/Incisional Hernia disrupts this Equilibrium PASSIVE UNLOADING of Lateral Abdominal Wall. DISUSE ATROPHY
Dubay and Franz, et al.Annals of Surgery, 2007 Implications: To what extent these biomechanical changes contribute to hernia recurrence is unknown. Are these changes potentially reversible with anatomic reconstruction that restores normal abdominal wall loading? Healed Laparotomy Group (Sham) – Intermediate biomechanical changes – decreased abdominal wall loading due to pain and decreased activity?
25 Breast reconstruction patients Single-pedicle TRAM – 14 patients Free TRAM – 9 patients Bilateral Free TRAM – 2 patients B200 IsostationTriaxial Dynamometer
Kind, et al. 1997 Greatest decrease in performance seen at 6 weeks Post Op Maximum Isometric Flexion Torque at 6 weeks (% of baseline): Pedicle TRAM; 58+/-10% Unilateral Free TRAM; 87+/-11% At 6 months (% of baseline): 89+/-13% 93+/-8% Conclusions: Loss of a Rectus muscle is ultimately well-tolerated clinically. Pedicle TRAM flaps cause a greater insult to the abdominal wall than Free flap technique.
21 patients 15 Bilateral Pedicle TRAM 6 Unilateral Pedicle TRAM Evaluated Preop and 1 Year Post Op Questionaire and B200 Isostation Dynamometer
Bilateral Pedicled Flaps Dulin, et al.
Unilateral Pedicled Flaps Dulin, et al.
Abd. Wall Fxn - TRAM Historical Importance – First studies of abdominal wall function as a surgical outcome. Precedent for objective measurement of abdominal wall function as a means to compare different surgical techniques. ????? How does this apply to Ventral Hernia? What in the WORLD is a Dynamometer?
22 Patients – Components Separation Technique 2 Patients Evaluated Preoperatively and 6 months Postoperatively (Cybex Dynamometry) 40% Increase in Truncal Force Generation
30 Incisional Hernia Patients 16 – Open Repair (no mesh!%#$!) 14 – Laparoscopic Repair 12 Healthy Controls – no prior surgery Biodex Dynamometer
D. den Hartog, et al. 2010 Mean Torque/Weight for trunk flexion (N m/Kg) was signficantly higher in the control group than in the hernia group. Trunk flexion strength (N m/Kg) was not significantly different between the two types of hernia repair. But the Open Repair group had greater trunk flexion strength than the Lap. Group after adjustment for Gender
10 Healthy Volunteers 10 patients with ventral hernias (>10 cm) (recruited from the “wait list” for surgery) Test/retest reliability – 2 exams 1 week apart. Validity – Questionnaire and Self Assessment.
Dynamometer - Disadvantages Expensive Large & Cumbersome Access is Limited Complicated – need a dedicated physiotherapist Need for standardized program
10-Point Abdominal Wall Strength Score 2-Component Physical Exam “Double Leg Lowering” “Trunk Raising”
EPIC Lift Capacity Six-stage progressive test of lift capacity designed to evaluate persons with medical impairments. It allows evaluation of how much one can safely lift: Over what vertical distance? How frequently? For what period of time? Very clearly established safety protocol based on heart rate window monitoring and high-risk lifting styles as a means to stop testing.
Knuckle to Shoulder Floor to Knuckle Floor to Shoulder Knuckle to Shoulder (4X) Floor to Knuckle (4X) Floor to Shoulder (4X)
EPIC Lift Capacity VERY well-established Since 1993: More than 2,000 professionals have been trained in its use. More than 700 professionals have been certified as ELC evaluators and technicians. Data have been collected on > 3,500 healthy normal subjects. ELC results have never been successfully challenged in a court in the U.S. or Canada. There has not been a single report of injury while using it. Patented: U.S. # 5,848,594. www.epicrehab.com
Conclusions: The relationship of abdominal wall function to ventral hernia repair is largely unstudied . The effects of hernia repair on abdominal wall biomechanics will likely guide our treatment of hernias in the future.
Drew Reynolds, M.D. QUESTIONS????