Download
1 / 71
800 likes | 1.04k Views
Denver School of Nursing – ADN & BSN Programs Lecture: Fridays 3:00pm – 9:00pm No Laboratory component for this class. Pathophysiology. BIO 206 & 308 – Ch 4 – pH & Fluid Balance. CH 4. Fluid, Electro, pH Balance. Distribution of Body Fluids

E N D
Denver School of Nursing – ADN & BSN Programs Lecture: Fridays 3:00pm – 9:00pm No Laboratory component for this class Pathophysiology BIO 206 & 308 – Ch 4 – pH & Fluid Balance
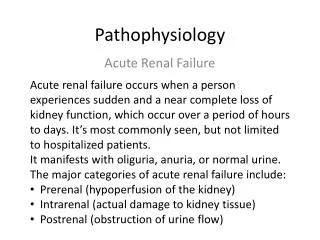
CH 4. Fluid, Electro, pH Balance Distribution of Body Fluids Total body water – all fluids 60% of weight Intracellular fluid (ICF) 2/3 TBW Extracellular fluid (ECF) 1/3 TBW • Interstitial fluid – between cells • Intravascular fluid – blood plasma • Lymph, synovial, intestinal, CSF, sweat, urine, pleural, peritoneal, pericardial and intraocular fluid
CH 4. Fluid, Electro, pH Balance “Cells live in a fluid environmentwith electrolytes and acid base concentrations maintained within a narrow range” changes or shifts → radically alter metabolism → life threatening
Sodium / Chloride Balance • Sodium (Na+) • Primary ECF cation • Regulates osmotic forces • Role • Neuromuscular irritability, acid-base balance, cellular reactions, and membrane transport • Chloride (Cl-) • Primary ECF anion • Provides electroneutrality
Fluid Balance Sodium and Water Balance Balance between Na+ and H2O - • ↑ or ↓ of salt • ↑ or ↓ water Tonicity– change in concentration of solutes (salt) with relation to solvent (water)
Fluid Balance Tonicity(280 – 294m Osm) • Isotonic – 0.9% NaCl – isoosmolar imbalance no change in cells • Hypertonic – ECF > 0.9% NaCl – (↓ H2O or ↑ salt) cells shrink • Hypotonic – ECF < 0.9% NaCl (↑ H2O or ↓ salt) cells swell “Extracellular Fluid”- interstitial space
Sodium (Na+) • 90% ECF cations • 135 – 145 mEq/L • Hypernatremia - > 145 mEq/L • Hyponatremia - < 135 mEq/L
Sodium (Na+) Hypernatremia-causes • ↑ Na or ↓ H2O • IV therapy – acidosis (NaHCO3) Cushing's Syndrome - ↑ ACTH → aldosterone fever, respiratory infection - ↓ H2O diabetes, diarrhea - ↓ H2O ↓ H2O intake - coma • H2O movement ICF → ECF(interstitial) • Manifestations • Intracellular dehydration: convulsions, thirst, fever, muscle twitching, hyperreflexia
Sodium (Na+) Hyponatremia • ↓ Na or ↑ H2O • Vomiting, diarrhea, GI suction, burns, diuretics, D5W replacement (isotonic sol’n) • Manifestations • Lethargy, confusion, depressed reflexes, seizures, coma, hypotension, tachycardia, ↓ urine output
Chloride (Cl-) Hypochloremia • Result of hyponatremia or ↑ HCO3 • Vomiting – loss HCl • Cystic fibrosis
Potassium (K+) Potassium (resting potential) • Major intracellularelectrolyte • 98% intracellular – Na – K – ATP Pump • 3.5 – 5.0 mEq/L • Transmission and conduction of nerve impulses, normal cardiac rhythm, skeletal and smooth muscle contractions: “action potentials” • “Da BAD BOY of ELECTROLYTES”
Potassium (K+) Potassium Levels • Change in pH affects K+balance Acidosis causes: ↑ ICF H+ → K+ moves out to ECF maintains + ion balance • Aldosterone; insulin, epinephrine Alkolosis causes: K+ → into cell • Glucagon # entry into cell Glucocorticoids → K+ excretion
Potassium (K+) Hypokalemia • K+ < 3.5 mEq/L • ↓ intake, ↑ loss, ↑ entry into cells • Manifestations: membrane hyperpolorizations↓ excitability – weakness, smooth muscle, atrophy, cardiac dysrhythmias (bradycardia…asystole)
Potassium (K+) Hyperkalemia • K+ > 5.0 mEq/L – rare • ↑ shift from ICF (acidosis), ↓ renal excretion, insulin deficiency or cell trauma
Potassium (K+) Hyperkalemia • Mild attacks • ↑ neuromuscular irritability – tingling of lips & fingers, restlessness, intestinal cramps – diarrhea • Severe attacks • No repolarization → muscle weakness, ↓ tone, flaccid paralysis • Cardiac dysrhythmias “funky chicken”
Calcium (Ca++) Calcium (threshold potential) • 99% located in bone – hydroxyapatite • Bone, teeth, blood clotting, hormone secretion, cell receptor function • Hypo - ↓ block of Na into cell ↑ neuromuscular excitability (muscle cramps) • Hyper - ↑ block Na - ↓ neuromuscular excitability (muscle weakness, cardiac arrest, kidney stones, constipation)
Calcium (Ca++) • Hypo - ↓ block of Na into cell ↑ neuromuscular excitability (muscle cramps) Source: Review of Clinical Signs, Dr. Frank Urbano MD 2007.
Big Picture… • Low SERUM K...decreased excitability • Nerves & muscles…bradycardia---asystole • High SERUM K …increased excitability • Cardiac dysrhythmias • Low SERUM Ca… increased excitability • “Chvostek & Trousseau’s Signs” • High SERUM Ca… decreased excitability
The Precious pH pH(0 to 14) • Inverse logarithm of the H+ concentration -0.0000001 mg/L – 1x10 -7 so pH = 7 • pH = power of hydrogen • pH changes by one unit (7 → 6) [H+] 10 fold • Biological fluids pH < 7.4 = acidic > 7.4 = basic Physiologic Range of Blood pH =7.35-7.45
pH Balance pH • Acids are formed as end products of protein, carbohydrate and fat metabolism • Narrow “life range” – 7.35 – 7.45 • Bone – lung – kidneys – major regulatory organs “Absolute Range of Life:6.8-7.8”
pH Balance pH • Body acids exist in two forms • Volatile H2CO3 (maybe eliminated as CO2) • Nonvolatile – eliminated by kidneys sulfuric, phosphoric
Ch. 29 Fluid & Electrolyte Balance • Image from: http://www.answers.com
Ch. 30 Acid-Base Balance • Image from: http://www3.oes.edu & http://www.fitnessspotlight.com
Fluid TUG of WAR!!! • Image from: http://www.getfit4kidz.com/
CH 4. Fluid, Electro, pH Balance Water Movement Between ICF and ECF “water, nutrients and waste products” capillary interstitial space • #1 Capillary hydrostatic pressure • blood pressure “fluid out” • #2 Capillary oncotic pressure • water attraction “fluid in”(Plasma Proteins) • #3 Interstitial hydrostatic pressure • fluid towards capillary • #4 Interstitial oncotic pressure • water attraction “fluid in”
water movement Source: Huether, McCance Understanding Pathophysiology 4th Ed. 2008
Edema Edema: 4 Major Causes “excessive accumulation of fluids within the interstitial space” • 1)↑ hydrostatic pressure • Venous obstruction – DVT, hepatic obstruction • Salt and water retention – heart, renal failure • 2)↓ plasma oncotic pressure • ↓ albumin– liver disease, malnutrition, kidney disease, burns, hemorrhage
Edema • 3)↑ capillary permeability – trauma, burns, neoplastic and allergic reactions • 4) Lymph obstruction – removal of nodes (surgery), inflammation or tumors
Source: Huether, McCance Understanding Pathophysiology 4th Ed. 2008
CH 4. Fluid, Electro, pH Balance • From your A&P sources… • What are the two most important body systems for fluid, Electrolyte, and pH balance??
CH 4. Fluid, Electro, pH Balance • What are the two most important regulatory systems for fluid, electrolyte and pH balance? • 1) • 2) • When the Blood pH is low, it is called? • When the Blood pH is high, it is called?
You have to know these 4 concepts / conditions to be a successful nurse! • 1) Metabolic Acidosis • 2) Metabolic Alkalosis • 3) Respiratory Acidosis • 4) Respiratory Alkalosis Much more detail to come latter in the lecture…
The Kidney • Image from: http://academic.kellogg.edu
The Renal Corpuscle • Image from: http://academic.kellogg.edu
Ch. 28 Urinary System • Physiology of the Urinary System: • Renal function • Filtration • Reabsorption • Secretion • Regulation of Urine Volume • Renin Angiotensin Aldosterone system (RAAS)
Urinary Physiology • Image from: http://www.answers.com
Fluid Balance Sodium, Chloride & Water Balance “kidneys and hormones” – central role • Water : ADH– hypothalamus – posterior pituitary • Na+ and Cl- • aldosterone – adrenal gland • Natriuretic hormones– atrial muscle
Acid-Base Balance Physiological pH Control Systems- (p.1003 of our text)
Acid-Base Balance The Chief Blood Buffer is a Mixture of Bicarbonate and Carbon Dioxide ~ All body fluids, inside or outside cells have buffers which defend the body against pH changes ~ The most important buffer in extracellular fluids, including blood, is a mixture of carbon dioxide (CO2) and bicarbonate anion (HCO3) ~ CO2 acts as an acid (it forms carbonic acid when it dissolves in water), donating hydrogen ions when they are needed ~ HCO3 is a base, soaking up hydrogen ions when there are too many of them ~ The HCO3/CO2 buffer system is extremely important because it can be rapidly readjusted in alkalosis and acidosis ~ There are also other buffers in blood, such as proteins and phosphate ~ The ability to resist pH change is given by the buffer capacity, which is a function of the concentration and dissociation constant (pK) of the weak acid ~ If there is more than one buffer in the solution, the buffer capacities are additive • Source: http://www.mpoullis.net
Acid-Base Balance • Source Mayo Clinic: http://discoverysedge.mayo.edu
Acid-Base Balance The Chief Blood Buffer is a Mixture of Bicarbonate and Carbon Dioxide • Source: http://www.mpoullis.net
Acid-Base Balance Too Much CO2 or Too Little HCO3 Will Cause Acidosis ~ The balance will swing toward a low pH, producing acidosis ~ Pathology leading to this Acidosis can be: 1) CO2 increase via hypoventilation (pneumonia, emphysema) 2) Metabolic conditions (ketoacidosis due to excess fat metabolism (diabetes mellitus) which will lower bicarbonate. • Source: http://www.mpoullis.net
Acid-Base Balance Too Much HCO3or Too Little CO2 Will Cause Alkalosis ~ The balance will swing toward a high pH, producing alkalosis ~ Pathology leading to this Alkalosis can be: 1) CO2 decrease via hyperventilation (Remember Respiration “Blows off CO2”) 2) Emesis removed stomach acid and raises bicarbonate (Alkalosis is clinically less common than acidosis) • Source: http://www.mpoullis.net