Download
1 / 49
490 likes | 851 Views
LOW MOLECULAR WEIGHT HEPARIN : BASIC & APPLIED ASPECT. Seminar Guide Dr. Rajkondawar. Introduction : New Generation heparin Prepared from enzymatic and chemical depolymerisation of unfractionated heparin (UFH) Mean molecular weight of 4000 - 6000 IU.

E N D
LOW MOLECULAR WEIGHT HEPARIN : BASIC & APPLIED ASPECT Seminar Guide Dr. Rajkondawar
Introduction : • New Generation heparin • Prepared from enzymatic and chemical depolymerisation of unfractionated heparin (UFH) • Mean molecular weight of 4000 - 6000 IU. • Heparin fragments can only bind to antithrombin - III when MW exceeds 5000 IU. • LMWH cannot bind to antithrombin - III and thrombin simultaneously. • But can bind to antithrombin - III and factor Xa. • Efficacy of the different LMWH depends upon difference in MW.
COMPARISON OF LOW M OLECULAR WEIGHT HEPARIN PREPARATIONS
Mechanism of Action: The Coagulation Cascade • Central to the coagulation cascade is the generation of thrombin (factor IIa) • thrombin is generated from prothrombin by the action of activated factor X (Xa) • thrombin then acts on fibrinogen to generate fibrin clot
Coagulation Cascade Intrinsic Pathway (surface contact) Extrinsic Pathway (tissue factor) XIIa VIIa XIa Heparin / LMWH(AT-III dependent) IXa Hirudin/Hirulog(direct antithrombin) Xa aPTT Thrombin (IIa) PT Thrombin-Fibrin Clot Coumarins Courtesy of VTI
Both UFH and LMWH exert their anticoagulation activity by catalyzing antithrombin(AT or AT III) • Catalyzed AT is accelerated in its inactivation of the coagulation enzymes thrombin (factor IIa) and factor IXa, Xa, XIa. • Prolongs aPTT (in case of UFH) • No prolongation of aPTT (in case of LMWH)
F F H H Thrombin Thrombin S S C C INTERACTION OF HEPARIN CO-FACTORS WITH THROMBIN Heparin has a higher affinity for AT than for HC II and there is more AT in plasma than HC II AT HC II ++++ - - - -
F H Thrombin S C ANTITHROMBIN AND FREE THROMBIN AT alone does not inactivate free-thrombin Free Thrombin AT
F H Thrombin S C INACTIVATION OF THROMBIN BYHEPARIN-AT COMPLEXES Heparin AT Heparin binds to antithrombin and increases the rate of thrombin inactivation
F H Thrombin S C EFFECT OF ANTITHROMBIN ON FIBRIN-BOUND THROMBIN The rate at which AT inactivates fibrin-bound thrombin is reduced 50-fold Fibrin-Bound Thrombin AT
LMWH UFH Inhibition of thrombin requires simultaneous binding of heparin to AT-III through the unique pentasaccharide sequence and binding to thrombin through a minimum of 13 additional saccharide units. Inhibition of factor Xa (Xa) requires binding heparin to AT-III through the unique pentasaccharide without the additional requirements for binding to Xa. 5 indicates unique high-affinity pentasaccharide.
PHARMACO KINETICS OF LMWH: • Usually administered by subcutaneous route. • Peak plasma level reached after 3 to 4 hours. • Does not bind to plasma proteins. • Plasma half life is 3 - 4 hours. • Rate of clearance from body is inversely proportional to molecular weight. • Cleared by renal excretion. • No hepatic metabolism.
MECHANISMS RESPONSIBLE FOR THE PHARMACOKINETIC ADVANTAGES OF LOW OLECULAR WEIGHT HEPARINS OVER UNFRACTIONATED HEPARIN
Clinical Indications : • Prophylaxis and treatment of venous thromboembolism. • Prophylaxis and treatment of pulmonary embolism. • Management of unstable angina (non-Q MI). • Acute thrombotic stroke. • Patency of coronary artery bypass graft. • Patency of femoro popliteal graft. • Post STK in cases of MI. • Before and after PTCA with or without stent.
General Surgery : At least as effective as low-dose unfractionated heparin but can be given once daily and cause fewer hematomas at injection sites. Low risk (Minor surgery, duration < 30 minutes.) Dalteparin, 2500 U 1–2 hr before surgery and once daily after surgery Enoxaparin, 2000 U 1–2 hr before surgery and once daily after surgery Nadroparin, 3100 U 2 hr before surgery and once daily after surgery Tinzaparin, 3500 U 2 hr before surgery and once daily after surgery High risk (Major abdominoperineal surgery gynaec, duration > 30 minutes.) Dalteparin, 5000 U 10–12 hr before surgery and once daily after surgery Enoxaparin, 4000 U 10–12 hr before surgery and once daily after surgery Ardeparin, 50 U/kg twice daily starting 12–24 hr after surgery
Orthopaedic Surgery : (THR, TKR, Hip fracture) • More effective than low-dose unfractionated heparin; more effective than warfarin in patients undergoing total knee replacement; no monitoring required. • Ardeparin, 50 U/kg twice daily starting 12–24 hr after surgery • Dalteparin, 5000 U 8–12 hr before surgery and once daily starting 12 hr after surgery • Enoxaparin, 3000 U twice daily starting 12–24 hr after surgery or 4000 Uonce daily starting 10–12 hr before surgery • Nadroparin, 40 U/kg starting 2 hr before surgery and once daily after surgery for 3 days; the dose is then increased to 60 U/kg once daily • Tinzaparin, 50 U/kg 2 hr before surgery and once daily after surgery or 75 U/kg once daily starting 12–24 hr after surgery.
Incidence of DVT in hip fracture is 43% and mortality is 12% when thromboprophylaxis is not given. • Colour doppler study for DVT has a low sensitivity and many patients can have asymptomatic DVT. So prophylaxis is always indicated. • Incidence of DVT is higher in total knee replacement Vs. THR. • Decreased incidence of intraop. bleeding with LMWH Vs. UFH. • Incidence of postop. bleeding can be by giving LMWH 8 - 12 hrs. before surgery. • Incidence of wound haematoma is considerably decreased by use of LMWH Vs. UFH. • Incidence of fatal pulmonary embolism decreased by 50%.
Acute Spinal Injury : • Incidence of DVT is 40%. • Maximum incidence in first 14 days. • UFH are associated with risk of bleeding. • LMWH + intermittent pneumatic compression is the treatment of choice. • Apparently effective whereas low-dose unfractionated heparin is not, and higher doses of unfractionated heparin cause excessive bleeding. • Enoxaparin, 3000 U twice daily • Multi Trauma : • LMWH risk of venous thrombosis from 44% to 31% and incidence of proximal vein thrombosis from 15% - 06%. • More effective than unfractionated heparin. • Enoxaparin, 3000 U twice daily
Medical Conditions: • Incidence of DVT in paralyzed limb in patient of ishaemic stroke is 42%. • As effective as low-dose unfractionated heparin but can be given once daily. • Dalteparin, 2500 U once daily • Enoxaparin, 2000 U once daily Patency of femoropopliteal bypass graft: • Graft survival at first year is 78% with LMWH Vs. Aspirin + Dipyridamole.
Treatment of Venous Thromboembolism : • Aims of treatment : • To prevent propagation of thrombus. • To stabilize the thrombus. • To prevent embolisation. • To promote recalnalisation. • LMWH have been found to be equally safe and more effective than UFH. • In few selected patient with DVT can be treated with LMWH on OPD basis. • LMWH can be a good alternative to Warfarin in high risk patients like pregnancy or patient with major bleeding, in secondary prophylaxis of DVT.
Venous thromboembolism : • At least as safe and effective as unfractionated heparinbut can be given subcutaneously without laboratory monitoring, thereby allowing treatment on OPD basis. • Dalteparin, 100 U/kg twice daily • Enoxaparin, 100 U/kg twice daily • Nadroparin, 90 U/kg twice daily • Tinzaparin, 175 U/kg once daily • Unstable Angina : • At least as effective as unfractionated heparin but can be given subcutaneously without monitoring. • Dalteparin, 100 U/kg twice daily • Enoxaparin, 100 U/kg twice daily • Recent Trial : • First Dose : Enoxaprin 30 mg IV bolus followed by 1mg/kg SC. bd. • (First dose 8 hrs. after IV bolus)
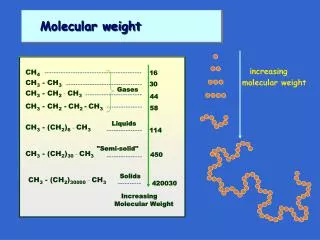
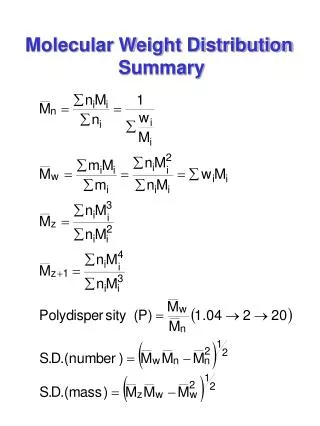
Factors Determining efficacyof LMWH : • Molecular weight • Inhibitory activity against thrombin and factor Xa • Extent of plasma protein banding • Plasma half life Relationship Between Molecular Weight and Anticoagulant Activity of Heparin Fractions
As the no. of oligosaccharides increases and mol. wt. increases - antithrombin activity increases Therefore heparin with highest mol. wt. has highest antithrombin activity Minimum of 18 saccharides chain length is required to form a complex with antithrombin
Montoring of LMWH 1. Usually not indicated 2. Required under two conditions a) Obese patient b) Patient with renal failure c) Patient on hemodialysis 3. Cromogenic anti Xa assay 4. Exact cut off value has not been determined but value > 0.8 U/Ml is associated with increased bleeding tendency 4. Target range of peak antifactor Xa is (i) 0.85 IU/ml for Tinzaparin. (ii) 1.3 IU/ml for Nadroparin. (iii) 1.05 IU/ml for dalteparin. 5. Best time to perform anti Xa assay is 4 hrs after SC. injection. 6. For twice daily administration, range is 0.6 to 1.0 U/ml 7. Frequent monitoring of anti Xa in patient with renal failure
Complications of LMWH therapy • 1. Bleeding tendency • Usually uncommon • Seen in patient with renal failure with GFR < 30 ml/min. • Treatment: • Protamine sulfate - unproven efficassy • It neutralises anti thrombin activity of LMWH but fails to neutralises ant factor Xa activity • Within 8 hrs of administration of LMWH - 1 mg. of protamin / 1mg of LMWH (or 100 anti Xa unit) • If bleeding still persists then - 0.5 mg / 1 mg of LMWH can be repeated after 4 hrs. • Smaller doses are required beyond 8 hrs.
2. HIT syndrome • Uncommon with LMWH • Suspected when platelet count falls by > then 50% or below 1.5 lac / cumm Bleeding menifestation at injection site Usually occurs on 5th day • Treatment • a) Danaparoids - Ant factor Xa activity • Monitoring by antifactor Xa assay • b) Direct thrombin inhibitor - Lepirudin • Bivalirudin • Argatroban • Ximelagatran • Monitored by aPTT • Special monitoring in patient with renal failure • Argatroban doses decreased in hepatic failure • No role of platelet transfusion
TREATMENT PROTOCOLS FOR DANAPAROID, LEPIRUDIN, AND ARGATROBAN
3. Osteoporosis • Uncommon with LMWH • Common with heparin in pregnancy, prosthetic cardiac valve, patient with anti phospholipid antibodies. • Significant reduction in bone density occurs in 30% of patients. • Symptomatic vertebral fracture occurs in 2-3% of patients. Mechanism • rate of bone formation. • bone resorption.
LMWH UNDER SPECIAL CIRCUMSTANCES • Obesity • Dose of LMWH is - U/kg. wt. • Obese person may have large TBW but have normal intravascular volume. • So theoretically there is a risk of bleeding. • In a meta analysis of data on 921 patients with BMI > 30 there was no increase risk of bleeding. • However, dose reduction can be consider when antifactor Xa level is high.
Renal insufficiency : • A linear co-relation between Cr. clearance and antifactor Xa level (p < 0.0003) in patient with Cr. clearance rate of < 30 ml/min. • Antifactor Xa activity increases in patients with renal function. • Pharmacokinetics effect may differ among various LMWH. • There is not a single Cr. clearance cut off value that co-relates with risk of bleeding. • So in patients with severe renal insufficiency it is safer to use UFH. • However LMWH does not risk of bleeding in prophylactic dose.
ESSENCE TrialEfficacy and Safety of SubcutaneousEnoxaparin in non-Q-Wave Coronary Events Study • A randomized study comparing the clinical efficacy of UFH vs enoxaparin LMWH in 3171 patients with rest angina or non-Q-wave MI • at 30 days, there was a relative risk reduction of 15% -16% in the rate of death, MI, or refractory ischemia as compared to standard heparin
Enox Hep Incidence of death, MI, angina14 d 16.6% 19.8% p=.01930 d 19.8% 23.3% p=.016 Minor bleeding30 d 13.8% 8.8% p<.001 Major bleeding30 d 6.5% 7.0% NS Death alone14 d 2.2% 2.3% NS30 d 2.9% 3.6% NS ESSENCE Enoxaparin 1.0 mg/kg q 12 h subcutaneous Unstable Angina Non-Q Wave MI UFH5,000 U bolus + infaPTT 55-85 sec Acute Phase min 48h, max 8 Days 30 days
Economic Assessment of LMWH vs UFHResults from the ESSENCE Trail enoxaparin heparin Need for coronary angioplasty (initial) 15% 20% p=.04 coronary angioplasty (30d) 18% 22% p=.08 diagnostic cath (30d) 57% 63% p=.04 Initial hospitalizationmean drug cost in U.S.* $155 $80 mean total cost of care $11,857 $12,620mean duration of treatment 2.3 daysmutidose vial enoxaparin - 1 mg/kg at $0.38/mg
Fixed Dose placebo q 12 h TIMI 11B - Study Design Fixed Dose < 65 kg > 65 kg 40 mg 60 mg q 12 h Enoxaparin 30 mg IV bolus + 1.0 mg/kg q 12 h subcutaneous Unstable Angina Non-Q Wave MI UFH 70 U/kg IV bolus + 15U/Kg/h UFH IV Acute Phase min 72h, max 8 Days Chronic Phase 43 days
TIMI 11BLMWH in Unstable Angina • 4,021 pts with acute coronary syndrome • Two treatment groups: UFH: 70 U/kg bolus 15 u/kg/hr iv LMWH: 30 mg bolus 1 mg/kg s.q. bid • Primary endpoint(death, MI, urgent revascularization) 48-72 hr 26% 14 days 15% p<0.03
Meta-AnalysisESSENCE and TIMI 11B Primary endpoint Death / MI / Urgent Revscularization Odds ratio Risk Reduction p-val Day 8 0.71 21% 0.02 Day 14 0.79 21% 0.0005 Day 43 0.80 20% 0.0006 European Society of Cardiology - August 1998
Enoxaparin for UA and non-Q MI DOSAGE DURATIONFor the prevention of 1 mg/kg q12h SC minimum 2 days; usual duration ischemic complications with oral aspirin therapy of therapy: 2 to 8 daysof unstable angina and (100 to 325 mg once daily) non-Q-wave myocardialinfarction (MI) whenconcurrently administeredwith aspirin
HEPARIN RESISTANCE • Failure of UFH : Anticoagulant activity. • Antithrombotic activity. • When daily requirement of UFH > 35000 IU to keep aPTT 1.5 - 2. • Causes : • Heparin binding to plasma proteins, platelet endothelium, macrophages & acute phase reactant. • Antithrombin - III deficiency. • Raised level of factor VIII. • Hyperfibrinoginemia. • Drug induced - Aprotinin. Nitroglycerine.
FUTURE TRENDS • Oral heparin • Heparins are not normally absorbed from GI tract. • Some delivery agents (N acylated amino acids) have been synthesized that forms covalent bonds with heparin & facilitate its absorption across GI mucosa. Clinical trials are underway. • Possible antineoplastic effect of LMWH. Animal studies have shown that LMWH inhibits metastases and angiogenesis necessary for tumor growth.