Download
1 / 73

E N D
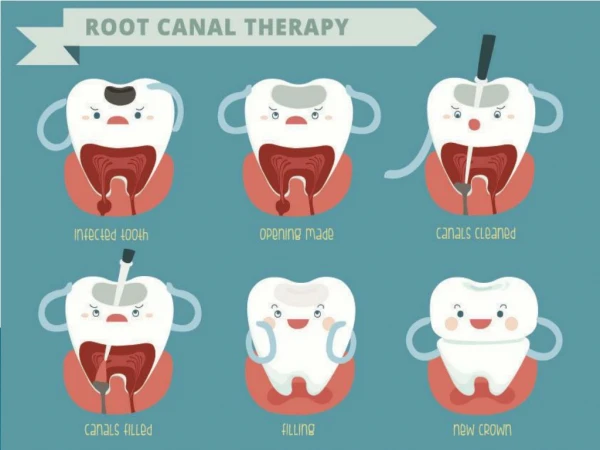
بسم الله الرحمن الرحيم Obturation of the Root Canal System Dr.Abdalazim Badraldin Sudanese Dental Center Khartoum – Sudan 26 March 2018
العمل الذي تحبه اخلص له اتقنه حتما ستصل لقمته • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Definition:- The Three-Dimensional Filling of the entire Root Canal System to or as close as possible to the Cemento-Dentinal Junction without gross overfilling or underfilling in the presence of a patent canal. • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
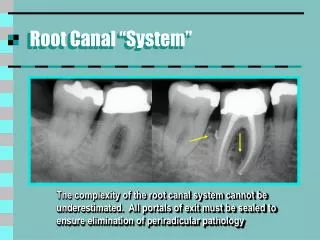
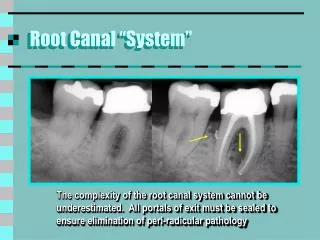
Obturation of Root Canal System Three Main Functions :- 1- Prevent Coronal Leakage of Microorganisms or potential Nutrients to support their Growth into the dead spaces of the Root Canal System. 2- Prevent Periapical or Periodontal Fluids percolating into the Root Canal System and Feeding Microorganisms . 3- Entomb any Residual Microorganisms that have Survived the Chemo-mechanical Instrumentation Stage of Treatment, in order to prevent their Proliferation and Pathogenicity . • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System • Objective :- ‘‘The total obturation of the root canal space, ‘‘in the final analysis, it is the sealing of the complex root canal system from the periodontal bone that ensures the health of the attachment apparatus against breakdown of endodontic origin.’ Dr. Herbert Schilder • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System SUCCESSFUL OBTURATION - Using of Materials and Techniques capable of Densely Filling the entire Root canals System. - Providing Fluid-tide Seal from the Apical Segment to Cavo- surface Margin of the Canal in order to Prevent Reinfection. • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Factors Influencing Complete Obturation :- 1- Quality of the Cleaning and Shaping of the Canal. 2- Skill and Experience of the clinician. 3- Materials and their Usage. 4- Restoration of the Tooth. 5- Health of the supporting Periodontium. • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System When to Obturate a Root Canal ? 1-Radicular space obturation is ideally accomplished after cleaning and shaping has been completed to an optimum size. 2-The canal(s) should be dry, with no ‘‘weeping’’ of fluids into the radicular space. 3-The tooth should ideally be asymptomatic. 4-There are also reports showing the importance of obturating canals following negative bacterial cultures. Sjogren et al. • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Apical Extent of Obturation ; Where & Why? -- Controversial ….No General Agreement. -- Canal obturation must stop at the cemento-dentinal junction,that corresponds to the maximal apical constriction. Grove 1929 -- Instrumentation and Obturation should be Contain within the Root Canal. Most North American & European Schools Cailleteau & Mullaney1997 - Ideal to Dentino-Cemental Junction without Overextension or overfilling. A-anatomic apex F-radiographic apex D-cemento-dentinal junction E-endodontic apex (apical foramen). • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System • The site of the cemento-dentinal junction is so variable that attempting to use it as a landmark is of little help to the endodontist. This junction often has unclear limits and can be found at different levels within the root canal. • Coolidge 1929 • It is also histologically impossible to find a point within the root canal where the pulpal tissue ends and the periodontal tissue begins. • Skillen WG. • Why root canal should be filled to the dentine-cemental junction • J Am Dent Assoc. 1930 • From a practical point of view it is not possible to use the cemento-dentinal • junction as a boundary of endodontic obturation. When • identified, more often than not, it is by chance.Orban B. • Why root canal should be filled to the dentino-cemental • junction. J Am Dent Assoc. 1930; Apical Extent of Obturation ; Where & Why? • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Apical Extent of Obturation ; Where & Why? • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System • The apical limit of canal instrumentation and obturation should not be the radiographic terminus of the canal, nor should it be the cemento-dentinal junction or the distance of 1 mm from the radiographic apex, but rather the • “apical constriction.” • This anatomical location, however, cannot be determined clinically with accuracy since it is “ever-changing. • Ricucci &Langeland • Apical limit of root canal instrumentation and obturation, • part 2. A histological study. Int Endod J.1998 Apical Extent of Obturation ; Where & Why? • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System • Relying on tactile sensation to locate the cemento-dentinal junction • can be misleading. The maximal constriction of the canal lumen may be due to the narrowing of the canal or to a calcification that may vary in distance from the true end of the endodontium. • Arnaldo Castellucci • Obturation of the Radicular Spaces Ingle’7 Apical Extent of Obturation ; Where & Why? • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System • Three-dimensionally obturated root canal as far as 0.5–1 mm from the radiographic terminus of the canal is in practice equivalent to having filled • it completely, leading to the success of the therapy. • Schiller 1987 Apical Extent of Obturation ; Where & Why? • The arbitrary rule that canal preparation should terminate 1 mm short of the radiographic apex should not be accepted in modern endodontic therapy. The “one millimeter” technique could result in instrumentation • short of the true canal terminus, possibly leaving necrotic and infected debris behind, leading to treatment failure. • Gutierrez JH, Aguayo P. • Apical foraminal openings in human teeth. Number and location. Oral • Surg Oral Med Oral Pathol Oral radiolEndod. 1995. • Blasković-Subat V, Maricić B, Sutalo J. • Asymmetry of the root canal foramen. Int Endod J. 1992 • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Apical Extent of Obturation ; Where & Why? Radiographic Terminus of the Canal • Because no one can insure sterility in any given root canal space, the surest chance of clinical success is gained when root canal systems, in all of their complexities, are filled to their full apical and lateral extents, • Peters et al • The difference between the “radiographic apex” and the “radiographic terminus of the canal” must be well understood. If the root canal is not straight and the foramen is on the distal, or on the mesial aspect of • the root, it is obvious that it has nothing to do with the “radiographic apex”, • therefore it makes no sense to advocate an instrumentation and then an • obturation .05 mm or more from the radiographic apex. • On the other hand, when the foramen in on the buccal or on the • lingual aspect of the root it is impossible to radiographically • see the terminus of the canal. • all of our endodontic treatments are performed at the • “electronic apex”, • Arnaldo Castellucci • Obturation of the Radicular Spaces • Ingle’7 • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Root Canal Filling Materials Divided into :- 1- Sealers( cements or Paste). 2- Root Filling Cements 3- Solid materials. 4- Semi-solid materials. Root Canal Sealers Sealers are self-hardening cements or paste used in conjunction with solid or semi-solid materials( that serve as the core of the obturation) to fill the empty spaces(voids) between these core materials and the canal walls. Most of the commercially available Endodontic sealers are resorbable within the root canal, so their use as the sole filling material is not recommended. • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Root Canal Filling Materials Sealer Root Canal Sealers Ideal sealers should be: • easily manipulated with ample working time • easily mixed in very fine powder particles and liquid form • tacky when mixed and adhesive to the canal walls when set • biocompatible and inert • physically stable (no shrinking after setting) • insoluble in tissue fluids • radiopaque • non-staining of tooth structure • bacteriostatic • easily removable with common solvents, if necessary • nonimmunogenic in the periapical tissues • neither mutagenic nor carcinogenic. • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Root Canal Filling Materials Sealer Root Canal Sealers • Functions or roles of root canal sealers • as antimicrobial agent • fill the discrepancies between the obturation materials and dentin walls • as binding agent • As lubricant • Give radiopacity • As canal obturating material • Classification of root canal sealers • 1-Sealers may be classified according to their composition (Ingle) • Eugenol • Non-eugenol • Medicated • Eugenol Root Canal Sealers • Basically the eugenol group may be divided into subgroup namely • a-silver containing • b - silver free • --- silver containing cements • Kerr sealer ( Rickert,1931) • -- Silver free cements • Grossman's sealer Tubliseal Wash's paste • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Root Canal Filling Materials Sealer Root Canal Sealers Non- eugenol Root Canal Sealers • Calcium Hydroxide –based Sealers SealApex,Apexit,Vitapex • Resin-based sealer AH26,AHPlus,Epiphany, Diaket • Solvent – based Sealers Chloropercha and eucapercha • Nogenol –based Sealer • Glass –ionomer-based sealers Ketac-Endo • Polycarboxylate-based sealers • Silicone-based Sealers Lee Endo-Fill, GuttaFlow • Calcium phosphate-based Sealers • Urethane Methacrylate - Based Sealers EndoRez • MTA-based Sealers ProRoot MTA • root canal sealers have therapeutic properties-usually • Used without core materials—Iodoform- disadvantages –compact root canal filling • Endofill • N2 • Endomethasone • Iodoform paste Medicated Root Canal Sealers • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Root Canal Sealers Grossman's sealer ( 1958) Composition : powered –zinc oxide 42 staybelite resin 27 bismuth subcarbonate 15 Barium sulfate 15 sodium borate 1 part liquid eugenol Properties it has plasticity and slow setting time due to the present of sodium borate Disadvantages –present of resin need vigorous spatulation other with it lodge on the canal wall Roth's 801( Roth's Pharmacy-Chicago) Grossman original formula .Roth only add bismuth subniterate instead of bismuth subcarbonate www.gvblack-krt.com
Root Canal Sealers • tg sealer(Technical&General) • According to • the manufacturer’s description, • Zinc Oxide- Eugenol Root canal sealer • Powder: • Zinc oxide---- Thymol –iodide ---Barium Sulphate • Liquid: • Eugenol • Advantages • does not( irritate) periapical tissues • Contains antiseptic and anti-inflammatory additives • Does not stain the tooth structure • Good radiopacity • High adhesion properties (Fluid-tight seal, not hermetic seal) • Easy of manipulation & application • acceptable work time www.gvblack-krt.com
Root Canal Sealers Zical According to the manufacturer’s description, Root Canal Sealant Based On Grossman's FormulaAntibacterial,non inflammatory * Root canal sealing using gutta percha points* Root canal sealing without using gutta percha points * Root canal filling for infected root canalsComposition:* Zinc Oxide * Bismuth Subcarbonate*Iodoform * Epoxy Resins* Barium Sulphate* Sodium borate Eugenol * Setting Time 5 - 10 Minutes* Working Time 4 - 6 SecondsProduct Benefits:* Antibacterial and non inflammatory* Based on Grossman's Formula* Radiopaque and non staining* Excellent thermal insulation
Root Canal Sealers • Endofill • According to • the manufacturer’s description, • Endofill is a radiopaque preparation for • permanent root-canal filling. • Its composition is well tolerated by tissues • and it provides anti-inflammatory, antiseptic • actions. Before hardening, the paste penetrates • the narrowest fissures and maintains its • therapeutic effects throughout the treatment • until completely set. The final • obturation neither retracts nor resorbs. • Endofill is available as REGULAR or SLOW setting • COMPOSITION • Powder :Dexamethasone Acetate 0.01%, • Hydrocortisone Acetate 1.0%, • Polyoxymethylene 2.2%, Thymol lodide 22.5%, • excipient ad 100% • Liquid :Eugenol www.gvblack-krt.com
Root Canal Sealers Calcium Hydroxide -Based Root canal Sealers SealApex (Sybron Endo/Kerr; Orange, Calif.) calcium hydroxide–paste to paste System. Base: zinc oxide, calcium hydroxide butyl benzene, sulfonamide zinc stearate. Catalyst : barium sulfate titanium dioxide as radiopacifiers resin, isobutyl salicylate, and aerocil. In 100% humidity, it takes up to 3 weeks to reach a final set. In a dry atmosphere, it never sets. the sealer expands while setting. Ingle question : Is SealApex soluble in tissue fluids to release the calcium hydroxide for its osteogenic effect? And if so, does this dissolution lead to an inadequate seal? LIFE (Sybron Endo/Kerr; Orange, Calif.) similar to SealApex Vitapex (NEO Dental, Japan) Contain 40% Iodoform Dentalis (DiaDent) Contain Iodoform& ZOE
Root Canal Sealers Resins -Based Root Canal Sealers Based more on resin chemistry AH-26 (Dentsply/Maillefer, Tulsa, Okla) ----Shroeder 1957 an epoxy resin. It is a glue, the base is biphenol A-epoxy. The catalyst is hexamethylene–tetramine. It also contains 60% bismuth oxide for radiographic contrast. As AH-26 sets, traces of formaldehyde are temporarily released, which initially makes it antibacterial. AH-26 is not sensitive to moisture and will even set under water. It will not set, however, if hydrogen peroxide is present. Properties– good adhesive property- good flow –antibacterial -it contracts slightly while hardening Low toxicity and well tolerated by periapical tissues. -The addition of a hardener ,hexamethylene tetramine,make s the cured resin Chemically and biologically inert. the setting time is 36 to 48 hours at body temperature and 5-7 days at room temperature. The Swiss manufacturers of AH-26 recommend that mixed AH-26 be warmed on a glass slab over an alcohol flame, which renders it less viscous. AH-26 is also sold worldwide as ThermaSeal(Dentsply/Tulsa; Tulsa, Okla.).
Root Canal Sealers AH PLUS Recognizing the advantages of AH-26 (high radiopacity, low solubility, slight shrinkage, and tissue compatibility) , as well as some of its disadvantages (formaldehyde release, extended setting time [24hours], and staining), the producers of AH26 set out to develop an improved product they renamed AH PLUS(Dentsply International). They retained the epoxy resin "glue” of AH26 but added new amines to maintain the natural color of the tooth. Its shade and color stability make it Material of choice where aesthetic demands are high. AH Plus comes in a paste–paste system, Paste A –epoxy resin -calcium tungstate -Zirconium Oxide -silica- -Iron Oxide Paste B – adamantaneamine-N,N-Dibenzyl-5-oxanonane-diamine- 1,9,TCD-diamine - Calcium Tungstate-Zirconium Oxide-Silica-Silicone oil
Root Canal Sealers • Properties: • has a working time of 4 hours and a setting time of 8 hours. • half the film thickness and half the solubility of regular AH26 • , and may be removed from the canal if necessary. • In a comparative toxicity study, AH Plus was found to be less • toxic than regular AH-26. -Easy to mix • -adapts closely to the walls of the prepared root canal • -Provides minimal shrinkage upon setting • -outstanding long- term dimensional stability and sealing properties. • Calcium release is absent due to absent of release of calcium hydroxide • Durarte et al in 2003 Suggested addition of 5 percent • calcium hydroxide so it leads to low viscosity material • As well as it provides a more alkaline pH and calcium release. • This higher alkalinity And enhanced calcium release leads to • improved biological and microbiological behavior, as a more • alkaline pH favors the deposition of mineralized tissue and exerts an • Antimicrobial action. • AH Plus is also sold worldwide as • ThermaSeal Plu (Dentsply/Tulsa; Tulsa, Okla.)-Ingel-5
Root Canal Sealers Glass ionomer –based Sealer Ketac-Endo (3M/Espe; Minneapolis, Minn.) Ease of manipulation radiopacity, Best bond to dentin, Fewest voids, Lowest surface tension, Best flow. Their greatest concern was the problem of removal in the event of re-treatment since there is no known solvent for glass ionomers . Experimental Sealer .
Root Canal Sealers Ceramic-based Sealers MTA-based Sealers ProRoot MTA: (Dentsply) Mineral Trioxide Aggregate - developed by Dr. torabinejad 1903 USA Composition white & Grey color Grey --- Tricalcium Silicate Dicalcium Silicate Bismuth Oxide Calcium Sulfate Tetracalcium aluminoferrite White ---- same as grey color except lack of tetracalcium alumino-ferrite Properties: -setting time 2 hours and 45 minutes. - pH 12.5 when set so it has biological & histological properties Similar to calcium hydroxide. -high compressive strength and produces hard setting non Resorbable surface. - it set in a moist environment (hydrophilic in nature –love of water) - low solubility -resistant to marginal leakage www.gvblack-krt.com
Root Canal Sealers - biocompatible - the mixture is a loose granular aggregate, so it doesn't stick to any instrument( cement 0r amalgam carrier),unless compacted very lightly the loosely bong aggregate will be pushed out of the cavity. -Bacteriostatic Disadvtages : - Difficult to manipulate - long setting time - costly Indication of use : - Apexification - Root resorptions - Root perforations - Pulp capping - Root end filling material ( grafting endodontic) Precautions : 1-MTA material should be kept in closed container to avoid moisture 2- should be stored in dry area 3- material should be immediately placed after mixing to prevent dehydration during setting 4- working time is about five minutes, if more time working is need The mixed material should be covered by moist gauge to prevent evaporation Or add small drop of water during capillary condensation technique. www.gvblack-krt.com
Root Canal Sealers Bio-Dentine • - Septodont.. September 2010 • Based on Active borosilicate Technology • Tri-calcium Silicate core • Designed to treat damage dentine- both for restorative( pulp capping) • and endodontic indications( perforation & open apex .root canal repair material). • Advantages:- • - Biocompatible… eliminates the risk of adverse tissue response. • - Help to preserve pulp vitality by promoting reactionary dentine genesis • - reduce the postoperative sensitivity by its outstanding sealing properties. • - Easy to use – need no surface condition or bonding. • - compactable strength • - quick setting • Usage :- • - deep class V cavities - gross root caries • - restore endodontic - access cavities • - indirect pulp capping - open apex
Root Canal Sealer Bio-Dentine Disadvantages:- 1- fast setting may lead to cracks in side the hardened biodentine 2-Have no long lasting antibacterial action (this action exist only during setting 10-12 m) Setting of biodentine is based on chemical reaction between CSC powder and CaCi2 which proceed fast. Slow setting ensures high pH which is maintained for along time.
Root Canal Sealers Nano-sized bioceramic sealer iRootSP(Innovative BioCreamix Inc, Vancouver, Canada) According to the manufacturer aluminum-free sealer based on a calcium silicate composition, Composition :- - calcium phosphate, -calcium silicates, -zirconium oxide, -calcium hydroxide. iRoot SP includes a similar composition to white mineral trioxide aggregate (MTA) iRoot SP can form a( hermetic) seal inside the root canal and be used for filling root canals with or without gutta-percha points., premixed, ready-to-use injectable white hydraulic cement paste developed for permanent root canal filling and sealing applications. iRoot SP is an insoluble, radiopaque, and aluminum-free material based on a calcium silicate composition, which requires the presence of water to set and harden. sealer is practically non resorbable bone-replacing bioceramic
Root Canal Sealers Properties: -Potent antibacterial activity , -absolute biocompatibility, -osseoconductivity, -ability to achieve excellent hermetic seal in constantly wet environment, -formation of chemical bond with dentin -insolubility in tissue fluids, -expansion during time of set, -very good radiopacity - easy handling iRootBP (Innovative BioCreamix Inc, Vancouver, Canada)iRoot® BP Injectable Root Canal Repair Filling Material (iRoot® BP) is a premixed injectable paste Composition: - Tricalcium Silicate - Dicalcium Silicate -Zirconium Oxide - Tantalum Pentaoxide -Calcium Sulfate iRoot® BP is packaged in a preloaded syringe and is supplied with disposable tips
Root Canal Sealers BioAggregate® (Innovative BioCreamix Inc, Vancouver, Canada) a new generation of a dental root canal repair filling material. BioAggregate® Root Canal Repair Filling Material (BioAggregate®) is a fine white hydraulic powder cement mixture for dental applications. It utilizes the advanced science of nano-technology to produce ceramic particles that upon reaction with water produce biocompatible and aluminum-free ceramic material. Composition:- Tricalcium silicate, Dicalcium silicate, Amorphous silicon oxide, Tantalum pentoxide, Calcium Phosphate monobasic www.gvblack-krt.com
Root Canal Filling Materials 1. Capable of being fully adapted to the prepared root canal walls 2. Dimensionally stable 3. Non-resorbable for an indefinite period of time 4. Non-irritating 5. Bacteriostatic, or at least should not encourage bacterial growth 6. Nonstaining to teeth 7. Preferably semisolid upon insertion and solid afterward 8. Capable of sealing canals laterally as well as apically 9. Impervious to moisture 10. Radiopaque 11. Sterile or sterilizable 12. Easily removed from the root canal, if necessary 13. Easily manipulable 14. Sticking to the canal walls 15. Nonconductor of thermal changes 16. Slightly expandable after placement 17. Able to set in a reasonable period of time. West JD. 1975 The relationship between the three-dimensional endodontic seal and endodontic failures Thesis, Boston University Ideal Properties of Obturating Materials • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Root Canal Filling Materials SOLID CORE MATERIAL SILVER POINT JASPER 1933 -- NO indication for their use today - widely used in the 1930s to the 1960s particularly in smaller canals - points, having the same diameter and taper as files and reamers ADVATAGES -Easy to insert - Length control was easier • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019 • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019 • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Root Canal Filling Materials SOLID CORE MATERIAL SILVER POINT DRAWBACK - Lack of plasticity lead to poor lateral and apical seal - cannot adequately fill all the canal space and cannot be compacted into spaces or voids within the root canal system -They maintain their round shape and no canal is perfectly round in shape, even after instrumentation. This leaves too much space to be filled by sealer or cement, thus leading to leakage. -The leakage allows corrosion of the silver points and the formation of silver salts. These products were found to be cytotoxic • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Root Canal Filling Materials SEMI SOLID CORE MATERIAL GUTTA PERCHA The composition of commercially available gutta-percha points consists of :- 18% to 22% gutta-percha, serves as the matrix 59% to 76% zinc oxide, Zinc oxide acts as the filler 1% to 4% waxes and resins, waxes and resins serve as plasticizers 1% to 18% metal sulfate (barium sulfate), provide the radiopacity to identify the material radiographically . • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Root Canal Filling Materials SEMI SOLID CORE MATERIAL GUTTA PERCHA The advantages of gutta-percha are: 1. It adapts to the canal walls because of its compatibility. 2. Once set, gutta-percha is stable in size. It shrinks only when chemically softened (e.g., with chloroform) following evaporation of the solvent, or if it is physically softened (e.g., by heat), during the cooling phase. For these reasons, chemical softening of gutta-percha is to be avoided, since it may create voids. Softening by physical means must be accompanied by compaction of the material to compensate for the volumetric changes that occur during the cooling phase. 3. Has a very low solubility rate. 4. It is well tolerated by tissues. 5. Weak bacteriostatic activity, attributed to zinc oxide. • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Root Canal Filling Materials SEMI SOLID CORE MATERIAL GUTTA PERCHA The advantages of gutta-percha are: 6. It is semi-solid when introduced in the canal. This allows easy manipulability. It becomes malleable if heated, so that it may assume any shape when compacted with appropriate instruments. This allows a three-dimensional filling of all canal spaces, both apical and laterally. 7. It is radiopaque because of its sulfate content (usually barium sulfate) and thus easily recognizable radiographically. 8. It can be easily disinfected. Immersion in 5%–6% sodium hypochlorite for 60 seconds . • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal System Root Canal Filling Materials SEMI SOLID CORE MATERIAL GUTTA PERCHA The advantages of gutta-percha are: 9. If necessary, it can be easily removed from the root canal when endodontic retreatment is indicated. 10. Gutta-percha is a poor heat conductor. 11. Once introduced into the root canal and heated, guttapercha expands. This characteristic helps to ensure a tighter seal, gutta-percha shrinks during the cooling phase; thus, to compensate for thermal shrinkage, any technique requiring heating must also include a compaction phase. SHORTAGES 1- Does not seal purely by itself (does not adhere to the dentinal wall), Sealing agents are necessary. 2- Lack of sufficient rigidity especially in small sizes; it cannot always be pushed beyond a ledge • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal SystemTECHENIQUES OF OBTURATION A- Cold lateral compaction method B. Warm vertical compaction method: 1. Touch ‘n’ heat 2. System B 3. EndoTwinn C. Thermocompactors: 1. New McSpadden nickel titanium thermocompacter 2. Maillefergutta condenser 3. Zipperer • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal SystemTECHENIQUES OF OBTURATION D. Canal Finder plugger (automated plugger) E. Thermoplasticized gutta-percha techniques: 1. Ultrafil 2. Obtura system 3. Pac 1600 4. Inject-R-FILL 5. Calamus flow obturation unit 6. Microseal system 7. Trifecta and successFil 8. Soft core obturation • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal SystemTECHENIQUES OF OBTURATION F. Ultrasonic plasticizing: 1. Cavitron with Pr-30 insert 2. ENAC G. Other systems: 1. Resilon 2. Gutta flow 3. Endo-Rez 4. Active GP system 5. Dentin chip apical filling • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal SystemTECHENIQUES OF OBTURATION LATERAL COLD COMPATION The most widely taught method of obturation of root canals in dental schools. canal must be prepared with a continuous tapered shape. The spreader used for lateral compaction should be placed within 1 to 2 mm of the working length. 1- Drying the canal 2- Placement of sealer 3- Placement of master cone 4- Obturation with Lateral Compaction placement of master cone spreader placement • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal SystemTECHENIQUES OF OBTURATION Advantages • Less technique sensitive, easy to manipulate. • No additional cost. Disadvantages • Time consuming. • More cones are required. • Canal irregularities are difficult to fill. • Chances of voids are more LATERAL COLD COMPATION spreader placement • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal SystemTECHENIQUES OF OBTURATION LATERAL COLD COMPATION • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal SystemTECHENIQUES OF OBTURATION 2. WARM VERTICAL COMPACTION METHOD • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019
Obturation of Root Canal SystemTECHENIQUES OF OBTURATION 2. WARM VERTICAL COMPACTION METHOD Touch ‘ n ‘ Heat an electronic device, especially developed for the warm vertical compaction of gutta-percha. The objective of this technique is to continuously and progressively carry a wave of warm gutta-percha along the length of the master cone starting coronally and ending apically • Dr.Abdalazim Badraldin • Sudanese Dental Center • Khartoum-Sudan • January 2019