Download
1 / 37
370 likes | 506 Views
Investigating IDA (BSG Guideline) And An overview of Obscure GI Bleed Dr.D.Ghosh Gastroenterology Registrar . Anaemia: <10-11.5g/dl for women <12.5-13.8g/dl for men

E N D
Investigating IDA (BSG Guideline) And An overview of Obscure GI Bleed Dr.D.Ghosh Gastroenterology Registrar
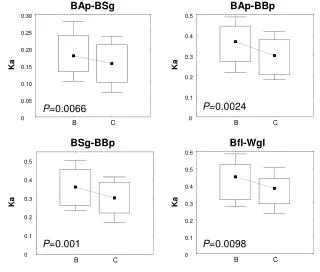
Anaemia: <10-11.5g/dl for women <12.5-13.8g/dl for men Not known at what level of Hb Ix should be initiated. No reason why mild anaemia should be less indicative of important disease than severe anaemia Iron deficiency: serum ferritin<12 MCV< 76 Transferrin sat<30% Bone marrow aspiration Therapeutic response Sr.transferrin receptor/ferritin ratio
Investigation History - dietary,drugs and family hx Examination-abd mass/cutaneous GI evaluation:all with confirmed IDA unless non GI blood loss Order of Ix in absence of symptoms-local availability OGD with small bowel bx : yield 30-50% Barium meal with coeliac serology if unable Colonoscopy:unless OGD positive for Ca or coeliac ALL pts should have lower GI ix Ba enema is a sufficent alternative with/without sigmoidoscopy (can omit in absence of lower GI symptoms and a normal PR Exam) FOB is of no benefit in the investigation of IDA –insensitive and nonspecific “The management of IDA is often suboptimal with most patients being incompletely investigated if at all”
Iron treatment • Different formulations • Vit c • Parental iron • Target: increase by 2 every 3wks • Replenish stores:3 more months • Monitor:3 monthly for a yr & then after one yr • Reassuring to know that IDA does not return in most pts in whom no cause is found after ix
Co-morbidity: appropriateness should be carefully considered and discussed with pts and carers. • Pre-menopausal women: • 5-10% incidence in that group • Hx unreliable to quantify • Ix only if>45yrs • Ogd & SI bx if upper GI symptoms • But coeliac serology in all • Lower GI ix only if symptoms,family hx,refractory after correction of potential cause • Post-gastrectomy:if refractory or occuring long after
Classification of vascular malformations that cause gastrointestinal hemorrhage
Small-bowel arteriovenous malformations as the cause of gastrointestinal hemorrhage
Small-bowel tumors as the cause of gastrointestinal hemorrhage
Gastrointestinal hemorrhage of obscure origin arising from small-bowel tumors
Types of nuclear medicine studies for the evaluation of small-bowel bleeding
Diagnostic yield of nuclear medicine studies for small-bowel bleeding
Enteroscopy in the diagnosis and management of small-bowel hemorrhage
Evaluation and management of chronic gastrointestinal bleeding of obscure origin






![[PDF] Free Download Broken - Sechs Geschichten By Don Winslow](https://cdn5.slideserve.com/9890698/slide1-dt.jpg)