Download
1 / 85
850 likes | 1.03k Views
Immune Function & HIV. dr shabeel pn. Inflammation. Response of vascular tissues to harmful stimuli i.e. pathogens, damaged cells, or irritants Protective attempt by the organism to remove injurious stimuli and initiate the healing process May be acute or chronic

E N D
Immune Function&HIV dr shabeel pn
Inflammation • Response of vascular tissues to harmful stimuli • i.e. pathogens, damaged cells, or irritants • Protective attempt by the organism to remove injurious stimuli and initiate the healing process • May be acute or chronic • Inflammatory response includes : • Vascular response • Cellular response • Formation of exudate • healing
Acute Inflammation • Short term process characterized by the classic signs of inflammation • Swelling • Redness • Pain • Heat • Predominant celltype: neutrophils
Chronic Inflammation • Lasts for weeks – years • Injurious agent persistent • Predominant cell type: lymphocytes and macrophages • Examples: • Autoimmune reactions • Rheumatoid arthritis • Prolonged exposure to chemical agents • silica
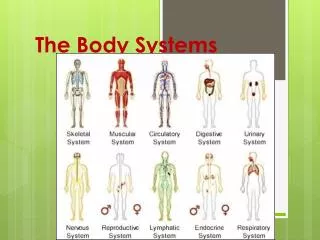
Immune system structures • The immune system protects the body from potentially harmful substances. The inflammatory response (inflammation) is part of innate immunity. It occurs when tissues are injured by bacteria, trauma, toxins, heat or any other cause.
Lymphoid Organs • Central lymphoid organs • Thymus • Bone marrow • Peripheral lymphoid organs • Tonsils • Gut-, genital-, bronchial-, & skin-associated lymphoid tissue • Lymph nodes • spleen
Normal Immune Response • Immunity • State of responsiveness to foreign substances such as microorganisms and tumor proteins • Types of Immunity • Active Acquired Immunity • Passive Acquired Immunity
Antigen • Large molecules (usually proteins) on the surface of cells, viruses, fungi or bacteria • Antibody • Protein produced by the immune system in response to the presence of an antigen
Antigens that get past the external barriers are targeted for destruction by the immune system
Antibodies • Attach to specific antigen • Make it easier for phagocytes to destroy antigen
Acquired Immunity • Is when the body is exposed to various antigens and builds a defense that is specific to that antigen
Passive Immunity • Antibodies that are produced in someone else's body • Infants have passive immunity because antibodies are transferred through the placenta from the mother • Last 6-12 months • Gamma globulin • Given IV, IM • Temporary protection
Aging and the Immune System • Decline in the immune system with aging • Characterized by higher incidence of tumors in elderly • Also seen with greater susceptibility to infections such as influenza and pneumonia
Altered Immune Response • Immunocompetence • immunity • Immunodeficiency diseases • Severe infections • Malignancies • immunity • Hypersensitivity disorders • Allergies • Autoimmune diseases
Hypersensitivity Reactions • Autoimmune Diseases • Four Types • Type 1, II, III are immediate and humoral • Type IV is a delayed hypersensitivity and cell-mediated
Type I Hypersensitivity Immediate/Anaphylactic Reactions • Occur in in susceptible people who are highly sensitized to specific allergens • Mediated by IgE antibodies • Release histamine and others by mast cells and basophils • Result in systemic inflammatory response (seconds to minutes) • Reaction can be local or systemic • Runny nose anaphylaxis • Mild irritation sudden death
Type I Hypersensitivity Reactions • Anaphylaxis • Immediate release of mediators • Injection • Bee sting • Reaction is within minutes • Can be life threatening • Bronchial constriction airway obstruction • Vascular collapse • Initial symptoms • Edema, itching at site of exposure • Can rapidly escalate into shock • Rapid weak pulse • Hypotension • Dyspnea • cyanosis • See Table 12-12
Anaphylactic Shock • Most severe type of anaphylaxis • From quick release of mast cells • Estimated 1.3-16.8% of population are “at risk” for having anaphylactic reaction especially to insect stings and penicillin (see table 13-11) • Results in ~1,000 deaths per year • Usually related to sudden cardiovascular collapse
Anaphylaxis • IgE acts to release histamine from mast cells • Histamine causes vasodilation of arterioles and constriction of bronchioles in lungs (bronchospasm) • Symptoms: Respiratory distress Unconsciousness Hypotension Urticaria (hives) Flushed appearance Angioedema (swelling of lips, face, throat) Anxiety Abdominal pain
Anaphylaxis • Life-threatening medical emergency d/t rapid constriction of the airway • Treatment • Epinephrine (adrenaline) • Β-2 adrenergic receptors -> powerful bronchodilator • EpiPen • May also cause tachycardia
Type I Hypersensitivity Reactions • Atopic reactions • Inherited tendency to become sensitive to environmental allergens • Allergic rhinitis (hay fever), asthma, dermatitis, urticaria
Type II: Cytotoxic and Cytolytic Reactions/ Antibody-Dependent Reactions • Antibodies produced by the immune system bind to antigens on pt’s own cell surface • Involve binding of IgG or IgM antibodies to antigens • Antigen-antibody complexes activate the complement system reaction/acute inflammation • Mediators of inflammation produce chemicals that lyse (destroy) cells (erythrocytes, platelets, leukocytes) • Hours to days • Examples • Hemolytic transfusion reactions • Goodpasture syndrome • Hashimoto’s thyroiditis
Hemolytic transfusion reactions • Results from ABO incompatibility • Antibodies coat the foreign erythrocytes agglutination occlusion of blood vessels • Cellular lysis • Acute renal failure
Type III: Immune-Complex Reactions • Results from antigen-antibody complexes • IgG, IgM complexes are deposited in tissue (kidneys, joints, lungs, small blood vessels) inflammation and cellular destruction • Local or systemic • Hours-days • Associated with systemic lupus erthymatosus (SLE), rheumatoid arthritis (RA)
Type IV: Delayed Hypersensitivity Reactions • Cell-mediated (not antibody-mediated) immune response causing tissue damage • Sensitized T lymphocytes attack antigens and release cytokines which attract macrophages • 2-3 days • Examples: • Contact dermatitis (poison ivy rash) • Transplant rejection
Allergic Disorders • Assessment • Health History • Physical Examination • Diagnostic Studies • Skin Tests • Procedure • Results • Precautions
Chronic Allergies • Characterized by chronic remissions and exacerbations • Allergen recognition and control • Skin testing • Elimination diet • Identification of aggravating factors • Medic Alert bracelet • Collaborative Care • Epi Pen • Antihistamines
Allergic Disorders (cont.) • Collaborative Care (cont.) • Drug Therapy • Antihistamines • Sympathomimetic/decongestant drugs • Corticosteroids • Antipruritic drugs • Mast cell-stabilizing drugs (cont.) • Immunotherapy • Mechanism of action • Method of administration
Systemic Lupus Erythematosus (SLE) • Chronic, mulitisystem inflammatory disease • Typically affects skin, joints, renal, hematologic, neurologic systems • Etiology: unknown • Autoimmune reactions are directed against host cells • Clinical manifestations are variable
SLE • Clinical Manifestations • Dermatological, M/S, Cardiopulmonary, Renal, Nervous system, Hematologic, Infection susceptibility
Polymysitis & Dermatomyositis • Diffuse, idiopathic, inflammatory myopathies of muscle weakness • Clinical manifestations • Fatigue, weakness • Classic cyanotic heliotrope rash • Joint pain • Diagnostic Studies • CK • ESR • Nursing Management • Assistive
Sjogren Syndrome • Autoimmune disorder that targets moisture producing glands dry mouth, dry eyes • Usually affects women over the age of 40 • “gritty” sensation of eyes • Symptomatic treatment
Immunodeficiency Disorders • Immune system does not adequately protect the body • Impairment of 1 or more immune mechanisms • Primary Immunodeficiency Disorders • Immune cells are improperly developed/absent • Secondary Immunodeficiency Disorders • Deficiency based on illness or treatment • Graft-versus-Host Disease • Transfusion or transplantation with immunocompetent cells
Immunosuppressive Therapy • Goal: adequately suppress immune response to prevent rejection while maintaining sufficient immunity to prevent overwhelming infection • Calcineurin Inhibitors • Sirolimus • Mycophenolate Mofetil • Polyclonal Antibodies (Antithymocyte Globulin and Antilymphocyte Globulin) • Monoclonal Antibodies • New Immunosuppressive Therapy
Corticosteroidal Therapy • AKA “steroids” • Prednisone • Solu-medrol • Discovered in 1948 • Believed to be “miracle cure” for arthritis • Used to relieve the signs, symptoms of many diseases • Long-term use leads to serious complications and side effects • Became known as “scaroids”
Corticosteroids • What Are They? • Corticosteroids are drugs closely related to cortisol, a hormone which is naturally produced in the adrenal cortex (the outer layer of the adrenal gland). • How Do They Work? • Corticosteroids act on the immune system by blocking the production of substances that trigger allergic and inflammatory actions, such as prostaglandins. However, they also impede the function of white blood cells which destroy foreign bodies and help keep the immune system functioning properly. The interference with white blood cell function yields a side effect of increased susceptibility to infection.
Corticosteroids • What Conditions Do They Treat? • Corticosteroids are widely used for many conditions. They are also used to control inflammation of the joints and organs in diseases such as: • rheumatoid arthritis • lupus (systemic lupus erythematosus) • ankylosing spondylitis • juvenile arthritis • inflammatory bowel disease • polymyositis • mixed connective tissue disease • polymyalgia rheumatica • scleroderma (systemic sclerosis) • vasculitis
Effects of Corticosteroids • Anti-inflammatory Action • circulating lymphocytes, monocytes and eosinophils • Inhibit accumulation of leukocytes at site of inflammation • Inhibit release of substances involved in inflammatory response • Therefore, suppress manifestations of inflammation (redness, tenderness, heat, swelling, local edema)
Effects of Corticosteroids cont’d • Immunosuppression • Cause atrophy of lymphoid tissue • Suppress cell-mediated immune responses • Decrease production of antibodies • Blood pressure • Vasoconstriction • Retention of Na (and water) • Carbohydrate and Protein Metabolism • Increase hepatic glycogenesis • Increase insulin resistance • Redistribute fat in cushingoid pattern
AIDS in the U.S. • Centers for Disease Control (CDC) estimated that in 2007 about 1 million people in US are living with HIV or AIDS • 46% estimated to be men who have sex with men • 31% estimated to be adults/adolescents infected through heterosexual contact • Blacks who make up 13% of population accounted for almost ½ of the number of HIV/AIDS cases diagnosed • In US and countries where latest therapies are available, many patients have been managing their HIV infection with antiretroviral therapy (ART) for more than 20 years.
AIDS Worldwide • The magnitude of the global HIV/AIDS epidemic vastly exceeds that in the United States. • At the end of 2001, more than 40 million people were estimated to be living with HIV/AIDS, and • More than 20 million had already died from AIDS. • Nearly three quarters of those with the disease are living in sub-Saharan Africa, where access to antiretroviral therapy is limited.
HIV and AIDS • The primary causative agent of AIDS is HIV • HIV infects lymphocytes and results in severe immunodeficiency. • Immunodeficiency can lead to infections, cancers and neurological manifestations.
The HIV Retrovirus • HIV retrovirus has a particular affinity for helper T lymphocytes (cells that control the functions of other immune cells) • Once inside T lymphocytes, HIV produces abnormal DNA and fuses with the cell’s normal DNA and takes over the cell’s machinery. • The invaded lymphocyte then produces HIV particles
The HIV Retrovirus cont’d • These viruses exit the dying cell and repeat the process in other T lymphocytes • Without treatment, T lymphocytes become depleted as HIV particles increase • The person develops an infection or malignancy
Transmission of HIV • Major routes of transmission • Through human blood • Including infected needles • Sexual Transmission • Through exchange of semen, vaginal and cervical fluids • Perinatal Transmission • During pregnancy, labor, delivery or breast-feeding
Disease Development • Typical course of HIV/AIDS is defined by three phases • Primary infection phase • Flu-like symptoms • Few days two weeks • Chronic asymptomatic/latency phase • Little or no symptoms of illness • Lasts average of 10 years • Overt AIDS phase • Occurs when person has a CD4 count < 200 mm3 (normal 800-1000 mm3) or • Development of an AIDS defining illness
HIV and AIDS • AIDS diagnosed when individual with HIV develops at least one of the following Table 14-1): • CD4+T count of less than 200 cells/µl Healthy adults have CD4+T count >1,000 • Development of opportunistic infection (OI) • Development of opportunistic cancer • Wasting syndrome • Loss of > 10% of total body mass • Development of dementia