Download
1 / 70
810 likes | 1.87k Views
Status Epilepticus. Stan Bernbaum MD CCFP-EM May 31, 2001. Outline - Status Epilepticus (SE). Case Presentation Definitions Epidemiology Clinical Features Causes / Outcomes Pathophysiology Management * General Drugs. CASE Patient BNW - 14 month female.

E N D
Status Epilepticus Stan Bernbaum MD CCFP-EM May 31, 2001
Outline - Status Epilepticus (SE) • Case Presentation • Definitions • Epidemiology • Clinical Features • Causes / Outcomes • Pathophysiology • Management * • General • Drugs
CASEPatient BNW - 14 month female PMH: -Recurrent Grand Mal seizures since birth, lasting up to 1 hour -On meds: Carbamazepine, Topiramate, & Clobazam -Family had detailed instructions from neurologist regarding management of her seizures HX: -Unwell all day- frequent vomiting, fever -Generalized tonic-clonic seizures began 1/2 hr ago -Presents to ER at PLC by EMS having generalized convulsions
CASE - continued P/E: -Generalized seizure activity, drooling, shallow respirations; being bagged by EMS -Pale, warm, diaphoretic -VS: P 180, R 28, T 40.3, Sat 88%
CASE - continued Management: AT HOME: -Had been given Lorazepam PR 0.1 mg/kg by father -EMS repeated Lorazepam PR, and also gave Midazolam IM 0.2 mg/kg -Glucometer by EMS - 7.2 -IV started just before arrival at hospital
CASE - continued MANAGEMENT IN EMERGENCY: -Bagging --> O2 sat 100% -Lorazepam 0.1 mg/kg IV -Phenytoin 20 mg/kg IV over 20 min -Acetaminophen 15 mg/kg supp -pt exposed to help cool -ABG, labs drawn ......still seizing
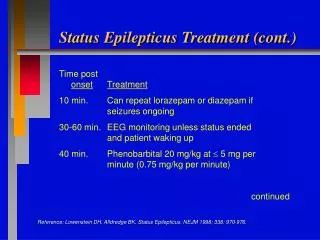
CASE - continued MANAGEMENT IN ER - continued: -Lorazepam 0.1 mg/kg repeat -consults - Peds PLC - Ped Neurologist and ICU @ ACH -O2 sat still 100% -ordered Phenobarbital 20 mg/kg IV ......still seizing
CASE - continued MANAGEMENT IN ER - continued: -ABG: pH 7.01 pCO2 elevated (other results not in chart) -Thiopental 5 mg/kg -Intubated (#5 uncuffed ET tube) ...... seizure activity stopped. -Phenobarbital given (from previous order)
CASE - continued MANAGEMENT IN ER - continued: repeat ABG: pH 7.4 pO2 359 sat 99 pCO2 18 HCO3 13 BE -9 Lactate 3.8 Gluc 8.3 CBC OK Na 144 K 3.2 Cl 108 CO2 12 A Gap = 24 -transferred to ACH ICU via transport team
Severe Myoclonic Epilepsy in Infants • recognized as a syndrome in 1982 • features: • family history of epilepsy or febrile convulsions • seizures begin during first year of life • very resistant to all treatment • unknown etiology • ataxia, pyramidal signs, & myoclonus develop • psychomotor development retarded from 2nd year • all have intellectual deficiency
Outline - Status Epilepticus (SE) • Case Presentation • Definitions • Epidemiology • Clinical Features • Causes / Outcomes • Pathophysiology • Management * • General • Drugs
Definition - Status Epilepticus • continuous or rapidly repeating seizures • no consensus on exact definition - “abn prolonged” • “no recovery between attacks” • “20-30 min” --> injury to CNS neurons • more practical definition: since isolated tonic - clonic seizures rarely last > few minutes ... consider Status if sz > 5 min or 2 discrete sz with no regaining of consciousness between • vs. serial sz - close together - regained consciousness in between
Outline - Status Epilepticus (SE) • Case Presentation • Definitions • Epidemiology • Clinical Features • Causes / Outcomes • Pathophysiology • Management * • General • Drugs
Epidemiology - SE • life threatening • USA: -102,000 -152,000 cases / year - 52,000 deaths / year • of new cases of epilepsy, 12 -30% present in Status • generalized Status is most common form - and subject of this review
Outline - Status Epilepticus (SE) • Case Presentation • Definitions • Epidemiology • Clinical Features • Causes / Outcomes • Pathophysiology • Management * • General • Drugs
Clinical - Generalized SE • at onset - usu obvious tonic / clonic • as continues often subtle - slight twitch of face / extremities, nystagmoid eye movements • may be NO observable motor sz ***still risk for CNS injury - assume still seizing if SE pt not waking • need EEG to definitely dx - not uncommon in comatose hospital inpatients
Outline - Status Epilepticus (SE) • Case Presentation • Definitions • Epidemiology • Clinical Features • Causes / Outcomes • Pathophysiology • Management * • General • Drugs
Outcome of SE • overall adult mortality 20% (>80 yr : 50%) • >90% mortality is d/t underlying disease • children - better outcomes - mortality 2.5 % • increase risk future SE / chronic sz • worse outcome if prolonged / severe physiologic disturbance • outcome depends on cause - acute vs chronic
Outcome of SE continued • Acute causes - difficult to control / higher mortality • sepsis - esp CNS • CNS - infx, stroke, head trauma, neoplasm • drug toxicity • hypoxia • metabolic encephalopathy • abn lytes, renal failure
Outcome of SE continued • Chronic causes - usu better response to Rx • known epilepsy - breakthrough sz +/- low anticonvulsant levels • ETOH / drug abuse / withdrawal • remote CNS process (eg brain surgery / CVA / trauma) --> SE after long latent period
Outline - Status Epilepticus (SE) • Case Presentation • Definitions • Epidemiology • Clinical Features • Causes / Outcomes • Pathophysiology • Management * • General • Drugs
Pathophysiology - SE • numerous mechanisms - poorly understood • failure of mechanisms that usu abort isolated sz • excess excitation or ineffective inhibition • there are excitatory and inhibitory receptors in the brain - activity is usually in balance
Pathophysiology - SE cont’d • GLUTAMATE = the major excitatory AA neurotransmitter in brain • any factor which increases Glutamate activity can lead to seizures • e.g. 1987- mussels contaminated with Domoic acid, a glutamate analog --> profound SE / deaths
Pathophysiology - SE continued • GABA = main inhibitory neurotransmitter • GABA antagonists can cause SE - eg Penicillins, other antibiotics • prolonged sz can desensitize GABA receptors
Pathophysiology - SE continued • CNS damage can occur - mechanism: • uncontrolled neuronal firing -> excess glutamate -> this sustained high influx of calcium ions into neurons leads to cell death (“excitotoxicity”) • GABA released to counteract this, but GABA receptors eventually desensitize • these effects worsened if hyperthermia, hypoxia, or hypotension
Pathophysiology - SE continued • PHASE 1 (0-30 min) -- compensatory mechanisms remain intact • adrenaline or noradrenaline release ++ • increased CBF & metabolism • hypertension, hyperpyrexia • hyperventilation, tachycardia • lactic acidosis
Pathophysiology - SE continued • PHASE 2 (>30 min) -- compensatory mechanisms failing • cerebral autoregulation fails / cerebral edema • respiration depressed • cardiac arrhythmias • hypotension • hypoglycemia, hyponatremia • renal failure, rhabdomyolysis, hyperthermia • DIC
Outline - Status Epilepticus (SE) • Case Presentation • Definitions • Epidemiology • Clinical Features • Causes / Outcomes • Pathophysiology • Management * • General • Drugs
OUTLINE - Management of SE • General approach • Anti - Epileptic Drugs: • Benzodiazepines • Phenytoin / Fosphenytoin • Barbiturates • Propofol • others / new possibilities
Management of SE • ABC’s (+ monitor / O2 / large IV’s) • START PHARMACOTHERAPY ASAP • Metabolic acidosis common - if severe, give Bicarb • if intubating / ventilating - avoid long-acting n-m blockers - masks sz activity • beware hyperthermia 2º sz - in 30-80% --> passive cooling
Management of SE continued • consider underlying causes: • infection (systemic / CNS) • structural: trauma, CVA, IC bleed • CNS malformations • metabolic - hypoxia, abn electrolytes, hypoglycemia • toxic - alcohol, other drugs • drug withdrawal - AED’s, benzos • congenital - inborn errors of metabolism
Management of SE continued • History & Physical - do once Rx initiated • Hx: events, trauma, meds, sz hx, ETOH, infx • P/E: Neuro - look for focal signs vs. generalized tonic-clonic • look for signs of underlying causes - trauma, infection, etc • LAB: gluc, lytes, creat, BUN, CBC, Ca, Mg, Phos, LFT’s, AED levels, ETOH / toxicology, PTT / INR -ABG
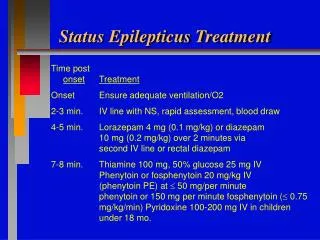
Management of SE continued • consider.... • Thiamine • Glucose • Pyridoxine 5 gm IV (70 mg/kg kids) • reverses INH action inhibiting GABA synthesis • now recommended routinely by NYC Poison Control in REFRACTORY SE d/t frequency of INH OD
OUTLINE - Management of SE • General approach • Anti - Epileptic Drugs: • Benzodiazepines • Phenytoin / Fosphenytoin • Barbiturates • Propofol • others / new possibilities
Drug Rx of SE • Starting Rx ASAP has been correlated with a better response rate to drug Rx, and lower morbidity • Lowenstein DH, Alldredge BK Neurology 1993 (43): 483-8 • < 30 min - 80% stopped • > 120 min - < 40% stopped but - retrospective review; ? groups comparable
Drug Rx of SE • Ideal agent characteristics: • easy to administer • prompt onset, long-acting • 100% effective vs seizures • no depression of cardio-resp function or mental status • no other adverse effects
Drug Rx of SE • Existing agents - adverse effects: • Benzos / Bbts - decrease LOC / respiration • Dilantin / (Fosphenytoin) - infusion rate-related hypotension / dysrhythmias • Dilantin / Bbts / (Fosphen) - slow onset d/t limited rate of administration
Drug Rx of SE • 1st - Benzodiazepines • * Lorazepam, Diazepam • 2nd - Phenytoin, Fosphenytoin • 3rd - Phenobarbital
Drug Rx - Refractory SE • Anesthetic doses of: • Midazolam (0.2 mg/kg slow IV bolus) - ->continuous IV infusion @ .4 - 6.0 mcg/kg/min OR .1 - 2.0 mg/kg/hr • Propofol (1-2 mg/kg) • Barbiturates (Thiopental, Phenobarbital, Pentobarbital) • Inhalational anesthetics (Isoflurane) • GA can suppress immune system -->infection
Non - IV Rx of SE • e.g. out of hospital -- often in children • Midazolam IM (or Intranasal) .15-.3 mg/kg • Diazepam Rectally .5 mg/kg (to 20 mg) • Lorazepam SL • (Paraldehyde rectally)
Lorazepam • 1st agent to use • Dose: Adults 4 -10 mg (.1 mg/kg) IV Peds .05 - .1 mg/kg (to 4 mg) IV • less lipid soluble than Diazepam --> smaller volume of distribution / longer T1/2 • effects last 12 - 24 hr • S/E: resp depression, hypotension, confusion, sedation (but less than diazepam)
Diazepam • Dose: Peds .1-1.0 (.2-.5) mg/kg IV • Adults 10 - 20 mg (.2 mg/kg) IV • Duration of action: < 1 hr
Midazolam • Dose: .2 mg/kg IV 5-10 mg IM 0.2 mg/kg Intranasal • Dose for refractory SE - continuous IV infusion @ .1 - 2.0 mg/kg/hr - titrated • Onset: IV 2 - 3 min / other routes 15 min • Duration: 1 - 4 hr
Phenytoin (Dilantin) • still the standard 2nd IV Rx after Benzo • dose: 18 - 20 mg/kg (better than “1 gram”) • IV solution is highly alkaline - dissolved in propylene glycol, alcohol, and NaOH - pH is 12 -give in large vein, dilute N/S, flush • rate: Š 50 mg / min (Peds: Š1 mg/kg/min) • onset of action: 10 - 30 min • duration of action: 12 - 24 hr
Phenytoin continued • S/E - (most avoided if slower administration) • hypotension • arrhythmias - (must monitor) • respiratory depression • venous irritation • extravasation -->tissue injury / necrosis • “purple glove syndrome”: progressive limb edema, discoloration and pain 2-12 hr post IV admin
Fosphenytoin • a prodrug of Phenytoin • it has no anticonvulsant action itself, but is rapidly converted to Phenytoin • Dosage: in “Phenytoin Equivalents” to attempt to avoid confusion • Molecular wt = 1.5 x Phenytoin ... so 1.5 mg Fosphen --> 1 mg Phenytoin • can safely give at 3x rate of Phenytoin, resulting in 2x amount of Phenytoin delivered
Fosphenytoin • Advantages over Phenytoin: • pH 8 (vs Phenytoin pH 12) • does not require solvent (Phenytoin is dissolved in propylene glycol) • can give IM when no IV access • IV: - less potential for irritation - can give faster - no risk of tissue necrosis if goes interstitial - does not precipitate in IV solutions • lower risk of hypotension and dysrhythmias
Fosphenytoin • Negative considerations: • COST Approx 20x that of Phenytoin • CONFUSION of ordering in “Phenytoin equivalents” • can give IV at rate of 150 PE/min, which delivers 100 mg/min of Phenytoin • 750 mg Fosphen = 500 mg PE - One UK hospital expresses orders in both units ie “500 mg PE (750 mg Fosphen)”
Fosphenytoin • confusion: • case report (Epilepsia 42(2): 288, 2001) - 25 yo female given infusion of Phenytoin (mistaken for Fosphenytoin) at 150 mg/min • bradycardia to 34 • BP dropped to 45/0 • asystole • oops. • resuscitated with CPR ( x 15 min), intubation, atropine, isoproterenol