Download
1 / 38
380 likes | 419 Views
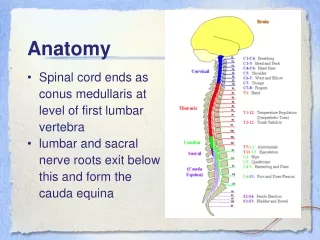
ANATOMY The optic nerve extends from the lamina cribrosa up to the optic chiasma . The nerve is covered by meningeal sheathes –the dura, the arachnoid and the pia . The subarachanoid space of the nerve is continuous with that of the brain .

E N D
ANATOMY The optic nerve extends from the lamina cribrosa up to the optic chiasma . The nerve is covered by meningeal sheathes –the dura, the arachnoid and the pia . The subarachanoid space of the nerve is continuous with that of the brain . The optic nerve consists of the axons of the ganglion cells of the retina i.e at the optic disk the fibers of the nerve fiber layer of the retina pass into the optic nerve .Behind the lamina cribrosa the nerve fibers are myelinated (or medullated).In front of the lamina cribrosa , the nerve fibers lose their myelin sheath and become transparent in the nerve fibers layer of the retina. The central retinal artery and vien pierce the memingeal sheathes around the optic nerve 10-12 mm behind the globe and then come to lie in the center of the nerve.
DISEASES OF THE OPTIC NERVE : Papilloedema (choked disk) : it is purely hydrostatic non inflammatory swelling of the optic disk (or nerve head) resulting from increased intracranial pressure and from obstruction to the orbital venous outflow . The condition is usually bilateral. However: • 1)One eye may be effected before the other . • 2)Degree of swelling may differ considerably in the two eyes.
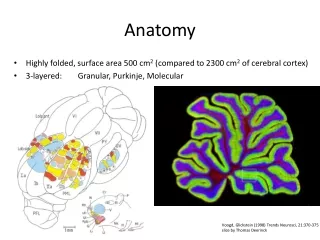
Normal optic nerve An optic nerve with mild swelling (papilledema).
Another example of an optic nerve with mild papilledema. The halo of edema now surrounds the optic disc.
Etiology: Increased intracranial pressure forces C.S.F into subarachnoid space around the optic nerve .Consequently the central retinal vien is compressed as it crosses the subarachnoid space while the thicker walled central retinal artery continues to transmit blood. As a result oedema of disk develops . I) Intracranial causes: 1)Tumours of brain (mid brain,barieto-occipital region and cerebellum ) are much the commonest cause and 80% of these are associated with papilloedema . The site of tumour is more important than its size. In general those tumours which tend to produce internal hydrocephalus will cause papilloedema .
Foster-Kennedy Syndrome :unilateral papilloedema with primary optic atrophy on the other side suggest a tumour of the opposite alfactory lobe or orbital surface of front lobe. 2) Cerebral abscess 3) Tuberculous or syphilitic meningitis 4) Cavernous sinus Thrombosis 5) Head injury with subarachnoid hemorrhage II)Systemic: • 1)Malignant hypertension • 2)Leukaemia Leukaemia
II) Systemic: 1)Malignant hypertension 2)Leukaemia III)Orbital: 1)Meningioma of optic nerve sheath 2)Orbital cellulites IV)Ocular: 1)Hypotony 2)Raised intraocular pressure as in acute congestive glaucoma. .
Symptoms: 1) For long vision – particularly central vision may be unimpaired. 2) Transient attacks of blurred vision due to spasm of retinal arteries. 3) When secondary optic atrophy sets in there is fall of vision and progressive contraction of visual field.
Sign The fundus picture is as follow : 1) in the early stage there is blurring and hyperaemia of the upper and lower margins of the optic disc: this extends around the nasal side then over the disc filling up The physiological cup the disc becomes elevated over the surrounding retina . By direct ophthalmoscopy adifference of 2-6d may be found between the focuss of the vessel at the top of the disc and those on the retina alittil way off 2) the veins are dilicated and tortuous their pulsation may be absent even on pressure Upon the globe .
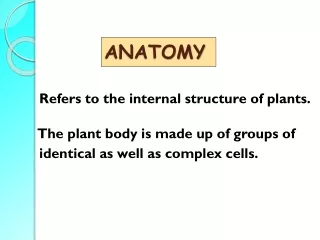
3) flame shaped haemorrhage and soft exudates are seen on and around the disc . 4) The radiating oedematos foldes around the macula take on the appearance of amacular fan or star . 5) post neurotic or secondary optic atrophy : the nerve fiber es unableto withstand the pressure degenerate 0 the disc become pale grey there is proliferation of fiberous tissue on the disc as aresult the margin are blurred and there is sheating of vessels. Differential diagnosis : • pseudo neuritis or pseudo papilloedema seen in cases of high hypermetropia or in astigmatism • Papillitis
Pseudopapilledema Papillitis
Treatment : The ideal treatment is the removal of the cause of raised intracranial pressure i.e. surgical removal of brain tumour . If this is not possible to retain vision decompression of the skull remove rigidity of skull bone burr hole or shunt operation is done . Once optic atrophy sets in visual prognosis becomes poor .
Optic neuritis: inflammation of the optic nerve Classification : 1-papillitis: when the optic disc or nerve head is inflamed . 2- retrobulbar neuritis : when the optic nerve behind the eyeball is inflamed. A -acute b -chronic –toxic amblyopic .
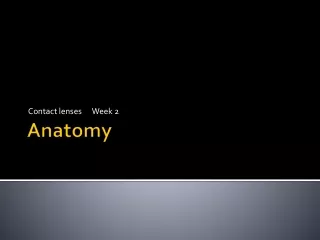
papillitis papillitis
Papilloedema. The disc is swollen and the disc margin has disappeared. The veins are congested.
Etiology : 1-septic foci teeth tonsilis sinusitis particularly of sphenoidal sinus and posterior ethmoidal cells since the optic nerve is closely related to them . 2- orbital cellulites 3- meningitis –tuberculous syphilitic . 4- choroio-retinitis –including sympathetic ophthalmitis 5- demyelinating diseases like disseminated or multiple sclerosis neuromyelitis optica (or Devic's disease ). Since the lesion in these diseases appear where the nerve fibers are myelinated the characteristic lesion in optic nerve is retrobulbar neuritis . 6- diabetes anaemia 7- lebers disease 8- exogenous toxins.
Symptoms: it is usually unilateral. 1) Sudden diminision of vision. 2)Pain on moving the eye upwards because of the attachment of the sheath of the superior rectus muscle to the sheath of the optic nerve near the optic foramen. Signs: 1) Ill sustained papillary reaction (Marcus Gunn pupil) inability to maintain contraction on prolonged stimulation with light
2) Fundus shows following picture. A) Papillitis: 1) Media is hazy due to exudation in vitreous. There is blurring and hyperaemia of the disc margin. Te physiological cup is obscured. The disc swelling is rarely more than 2-3 D. 2) The veins are dilated and tortuous. 3) There may be flame – shaped hemorrhages and soft exudates on and around the disc. 4) Post neurotic or secondary optic atrophy. Refer papilloedema B) Retrobulbar neuritis: The fundus appears normal. The condition may be truly defined as a disease wherein neither the ophthalmologist nor the patient sees anything! Differential diagnosis: refer papilloedema.
Treatment: 1-Treatment of cause such as septic focus sinusitis . 2-Corticosteroids –orally or by posterior subtenons injection. Recently, high dose of Methylprednisolone IV has been recommended. 3-Injection of high doses of vit. B1, B6, B12.
Chronic Retrobulbar Neuritis : (Toxic Amblyopic) It includes a number of conditions in which the ganglion cells/optic nerve fibers are damaged by the exogenous poisons. Etiology: 1-Tobacco-chewing or smoking. The causative agent is nicotine, collidine or lutidine. 2-Ethyl and methyl alcohol. 3-Lead 4-Arsenic 5-Quinine Predisposing factors: poor general health and vitamin deficiency.
Symptoms: 1) radual diminision of vision – sharp vision i.e. vision for fine work such as reading fine print, threading a needle ect. Is particularly affected. 2) Colour blindness. Sign: At first no changes are seen in the fundus.Later there is blurring of the disc margin, pallor of the temporal side of the disc. Central fields: shows central or centrocaecal scotoma for white and coloured objects (red and green).
Treatment: 1-Complete withdrawal of tobacco, alcohol 2-Administration of high doses of Vitamin B1 , B6 and B12 (hydrox-cobalamine) 3-Improvement of general health 4-Vasodilators – nicotinic acid.
OPTIC ATROPHY: It is a term usually applied to the condition of the optic disc when the optic nerve is degenerated. Etiology: 1-Syphilis – Tabes dorsalis, G.P.L. 2-Pressure – pituitary tumour , glioma of optic nerve 3-Tuberculous meningitis. 4-Glaucomatous optic atrophy 5-Circulatory optic atrophy – due to occlusion of central retinal artery, arterio- sclerosis. 6-Consecutive optic atrophy – due to destruction of ganglion cells in retina as in retinitis pigmentosa, choroiditis.
OPTIC ATROPHY Central Field Loss OPTIC ATROPHY
7-Traumatic optic atrophy: Avulsion of optic nerve. fracture of skull, heamorrhage into optic nerve sheath. 8-Toxic optic atrophy : exogenous toxins, tobacco alcohol , 9-Metabolic diabetes mellitus 10- Demyelinating disease – disseminated sclerosis , 11-Hereditary – Liber's disease. Pathology: 1-Columnar optic atrophy: occurs when degeneration and regeneration are orderly and the proliferating astrocytes arrange themselves in longitudinal columns replacing the nerve fiber layers. 2-No pattern optic atrophy occurs when there is replacement of the nerve fibers with glial tissue which is excessive and is densely tangled. 3-Cavernous optic atrophy occurs when there is degeneration of nerve fibers without much replacement by glial tissue .
Symptoms: 1-Usually there is progressive diminished of vision . 2-Colour blidness. Signs: 1-When atrophy is complete the pupil is dilated and fixed. 2-Fundus shows:
3)consecutive optic nerve atrophy : seen in retinitis pigmentosa, choroiditis. Disc: Yellow, waxy appearance, edge are well defined. Retina: vessels, show marked attenuation, particularly in case of retinitis pigmentosa. Surrounding retina shows evidence of retinitis pigmentosa, choroditis (pigmentary disturbance). Peripheral Fields: show concentric contraction or irregular or sector shaped defects. Treatment: 1-Directed at the cause –anti-syphilitic treatment penicillin in high doses , removal of pituitary tumour. 2-vasodilators: Tb. nicotinic acid. 3-Injection Vitamins B1, B12 in high doses.
MEDULATED NERVE FIBERS OR OPAQUE NERVE FIBERS: Medullation of the optic nerve fibers starts centrally i.e. from the brain and at birth reaches a level immediately behind the lamina cribrosa , normally the process ceases here . But occasionally patches of nerve fibers on the optic disc or in the retina region medullary sheath after they have passed through the lamina cribrosa . These are called medullated nerve fibers or opaque nerve fibers.
OPHTHALMOSCOPIC APPEARANCE: They appear as white patches with a feathery outline on and around the disc. Usually the retinal vessels are covered in places by opaque nerve fibers. Medullated nerve fibers disappear in cases of demyelinating diseases , optic atrophy due to pituitary tumour, glaucoma. Field defects: Opaque nerve fibers produce an enlarged blind spot or an arcuate scotoma.