Download

1 / 15
150 likes | 231 Views
Proposed changes to the way we inspect and regulate care services. 1. Our purpose and role. Our purpose We make sure health and social care services provide people with safe, effective, compassionate, high-quality care and we encourage care services to improve Our role

E N D
Proposed changes to the way we inspect and regulate care services 1
Our purpose and role Our purpose We make sure health and social care services provide people with safe, effective, compassionate, high-quality care and we encourage care services to improve Our role We monitor, inspect and regulate services to make sure they meet fundamental standards of quality and safety and we publish what we find, including performance ratings to help people choose care 2
Our direction • A strong, independent, expert inspectorate, evidence-based judgements • Always on the side of people who use services 3
Asking the right questions about quality and safety • Safe? • Effective? • Caring? • Responsive to people’s needs? • Well-led? 4
What will be different • FROM • Focus on Yes/No ‘compliance’ • A low and unclear bar • TO • Professional, intelligence-based judgements. • Ratings: Clear reports that talk about safe, effective, caring, well-led and responsive care • 28 regulations, 16 outcomes • Five key questions • On the side of people who use services. • Providers and commissioners clearly responsible for improvement. • CQC as part of the system with responsibility for improvement • Specialist with teams of experts. • Longer, thorough and people-focussed inspections. • Generalist inspectors • Generic inspections • Corporate body and registered manager held to account for the quality of care • Individuals at Board level also held to account for the quality of care. 5
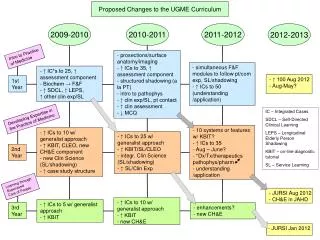
A New Start • Consultation launched June 2013 6
New Operating Model Surveillance
Registration • A more rigorous test to deliver safe, effective, compassionate, high-quality care • Legally binding • Named leaders held accountable Surveillance 8
Surveillance • Continuous monitoring to identify failures and risk of failure • “Smoke alarms” and “tin openers” • Use local and national information sources • Use qualitative information from people Surveillance Surveillance 9
Inspection • Chief Inspectors of Hospitals, Social Care, and General Practice • Expert inspection teams • Longer inspections, more time talking to people • Intelligence used to decide when, where and what to inspect • Inspectors using professional judgement Surveillance 10
Clear standards • Services must meet fundamentals of care and the expected standards • Three levels • Fundamentals of care • Expected standards of care • High quality care. Surveillance 11
The fundamentals of care – suggestions to promote debate • I will be cared for in a clean environment • I will be protected from abuse and discrimination • I will be protected from harm during my care and treatment • I will be given pain relief or other prescribed medication when I need it • When I am discharged my ongoing care will have been organised properly first • I will be helped to use the toilet and to wash when I need it • I will be given enough food and drink and helped to eat and drink if I need it • If I complain about my care, I will be listened to and not victimised as a result • I will not be held against my will, coerced or denied care and treatment without my consent or the proper legal authority 12
Ratings • Ratings for services as well as provider eg Maternity services • Ratings to help people choose between services and to encourage improvement. • Ratings for each? • Safe • Effective • Caring • Responsive to people’s needs • Well-led Surveillance 13
Taking action • Providers of care to be open and honest about issues affecting care – a duty of candour • New powers to: • Hold individuals accountable for poor care • Prosecute before issue of a formal warning first • Action in the NHS – phases: • Chief Inspector of Hospitals identifies failures and requires improvement • Special measures – programme for action by Monitor or NHS TDA to protect people and deal with the failure • Monitor or NHS TDA can dismiss the Board, and, if necessary, a special administrator appointed. In rare cases, the service may be closed 14
Questions for table top discussion • What do you think of the overall changes we are making? • Do you agree with the five questions we will ask? • What will be the impact on how you train and support staff? 15