Download
1 / 32
330 likes | 590 Views
Brain Injury in Premature Infants: The Role of Cerebral Autoregulation. Jeffrey R. Kaiser, MD, MA Pediatrics, Neonatology UAMS College of Medicine Little Rock, AR Perinatal Conference February 17, 2005. Background. Sick VLBW Infant.

E N D
Brain Injury in Premature Infants: The Role of Cerebral Autoregulation Jeffrey R. Kaiser, MD, MA Pediatrics, Neonatology UAMS College of Medicine Little Rock, AR Perinatal Conference February 17, 2005
Background Sick VLBW Infant Advances in obstetric & newborn intensive care over the last 4 decades have led to dramatic improvements in survival for the most premature of infants
Prematurity & Brain Injury →→ • The immaturity of the premature infant’s brain makes it inherently more vulnerable to injury • The more premature, the greater the chance of brain damage
The Magnitude of the Problem of Brain Injury in VLBW Infants More VLBW infants at risk of developing severe brain injury are now surviving • Large absolute number of VLBW infants affected (>55,000/year in U.S.) • High survival rates (>85%) • 15% of VLBW infants with severe brain injury
Causes of Brain Injury in the Premature Infant Multifactorial • Vascular: • Immature thin & fragile blood vessels can easily rupture • Extravascular: • Poor support for the blood vessels • Intravascular: • Blood clotting problems • Disturbed regulation of CBF & BP
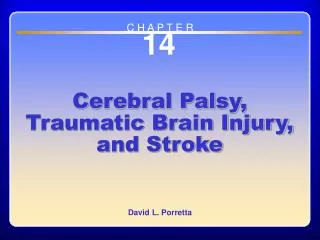
140 140 120 120 ) ) 1 1 - - Upper Upper Lower Lower min min 100 100 Limit Limit Limit Limit 1 1 - - 80 80 60 60 (ml•100 gm (ml•100 gm 40 40 Autoregulatory Plateau Autoregulatory Plateau 20 20 CBF CBF 0 0 20 20 40 40 60 60 80 80 100 100 Mean Carotid Arterial Blood Pressure Mean Carotid Arterial Blood Pressure (mm Hg) (mm Hg) Cerebral Autoregulation • Maintains constant blood flow to the brain despite wide changes in BP • Narrowing or dilation of terminal cerebral arterioles • Present in healthy adults, term newborns, fetal & neonatal lab animals Intact
Cerebral Autoregulation in Premature Infants • Cerebral autoregulation is generally considered impaired in sick premature infants (Lou, 1979) • Many premature newborns, however, have intact cerebral autoregulation (Kaiser, 2004, Tsuji, 2002) Pressure Passive (Impaired)
Significance If the pattern of cerebral autoregulation can be understood, then interventions to control fluctuations of BP, CBF, & ABGs could be implemented for VLBW infants in the hopes of preventing subsequent brain injury & long-term neurodevelopmental disability
Determination of Cerebral Autoregulatory Capacity • Instantaneous changes in CBF are compared to changes in BP after routine neonatal care procedures • Adult tests too invasive • Surfactant therapy & endotracheal tube suctioning
Experimental Protocol • Ventilated VLBW infants during the 1st week, no ultrasound evidence of brain injury prior to the study or major congenital anomalies • Baseline continuous monitoring of BP, O2, CO2, & CBF (~15 min) • Surfactant administration or ETT suctioning • Monitoring ≥ 45 min
Surfactant Administration Acutely Affects Cerebral Hemodynamics in VLBW Infants Kaiser JR, Gauss CH, Williams DK.Journal of Pediatrics, 2004.
Surfactant Therapy Affects BP, PaO2 & PaCO2 • Cerebral hemodynamics (contradictory results) • Increased • Decreased • Unchanged
Surfactant StudyObjectives • 1° Objective • Determine effects on CBF • Assess whether changes in CBF are primarily associated with changes in PaCO2 or BP • 2° Objective • Determine the presence or absence of cerebral autoregulation
Surfactant StudyHypothesis Significant increases in CBF occur briefly during surfactant administration that may be associated with brain injury in VLBW infants
CBF Velocity Measurement: Transcranial Doppler Ultrasound of the Middle Cerebral Artery
% Change From BaselineDuring Surfactant Administration MABP CBF PaCO2 PaO2 n=14
MABP’s Effect on the Cerebral Vasculature • Changes in MABP had much less impact on CBF than PaCO2 • In fact, a majority of infants displayed intact cerebral autoregulation--constant CBF with changes in MABP • 2 of 14 infants had ↑CBF that was associated with ↑ MABP (impaired autoregulation)
PaCO2’s Effect on the Cerebral Vasculature • Changes in PaCO2 highly associated with changes in CBF in VLBW infants • Consistent with PaCO2’s effect CBF CBF
The Effects of Hypercapnia on Cerebral Autoregulation of Ventilated VLBW Infants Jeffrey R. Kaiser, MD, MA C. Heath Gauss, MS D. Keith Williams, PhD In preparation, Pediatric Research
Pediatrics 1999;104:1082-88 • Permissive hypercapnia is being utilized in intubated VLBW infants to minimize ventilator-induced lung injury • The effects of permissive hypercapnia, (PaCO2, 45-55 mm Hg), on CBF and cerebral autoregulation as well as neurologic outcome of such infants have not been primarily examined (Mariana, et al, 1999)
Hypercapnia and Cerebral Autoregulation • Studies in animals and adults indicate the following: • Hypercapnia is associated with impaired autoregulation • Impaired autoregulation can be restored by hypocapnia
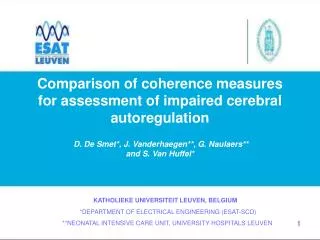
70 60 Upper Upper Lower Lower Limit Limit 50 Limit Limit 40 80 30 60 40 20 10 20 0 0 20 15 40 25 35 60 80 45 55 Cerebral Autoregulation in Preterm Infants CBF (cm/s) 40 30 MABP (mm Hg)
Hypercapnia StudyHypothesis Cerebral autoregulation in VLBW infants becomes progressively impaired with increasing PaCO2
Hypercapnia StudyObjective Examine the effects of increasing PaCO2 on the cerebral autoregulatory capacity of ventilated VLBW infants
Hypercapnia StudyStatistical Methods • The slope of the relationship between mean CBF velocity and MABP was estimated for all suctioning sessions (117, n = 43 VLBW infants) • BP range: 30-40 mm Hg • PaCO2 was statistically fixed at 30, 35, 40, 45, 50, 55, and 60 mm Hg • Slope near 0: intact cerebral autoregulation • Slope > 0: impaired cerebral autoregulation
Effects of Increasing PaCO2 on the Relationship between Mean CBF Velocity & MABP
Relationship between Highest PaCO2 in VLBW Infants in the Permissive Hypercapnia Era & IVH • No IVH 60.8 20.4 mm Hg • Grade 1 IVH 62.2 17.4 mm Hg • Grade 2 IVH 73.7 24.4 mm Hg • Grade 3 IVH 74.2 25.6 mm Hg • Grade 4 IVH 80.6 25.3 mm Hg P < 0.001, n = 995
Hypercapnia Study Conclusion • The slope of mean CBF velocity vs. MABP progressively increases with increasing PaCO2 • The cerebral circulation becomes more pressure- passive with increasing PaCO2
Hypercapnia StudySpeculation These novel data describing the effects of elevated PaCO2 on the capacity for cerebral autoregulation should raise concerns regarding the liberal use of permissive hypercapnea in VLBW infants during the first week of life
NINDS Gerald A. Dienel, PhD D. Keith Williams, PhD Heath Gauss, MS K.J.S. Anand, MBBS, DPhil Jeffrey M. Perlman, MD Robert W. Arrington, MD Neonatologists Carol Sikes, RN GCRC (M01RR14288) ACHRI, UAMS, and CUMG Foundations UAMS NICU Nurses & Respiratory Therapists Ultrasound Technicians Parents Acknowledgements