Download
1 / 31
310 likes | 466 Views
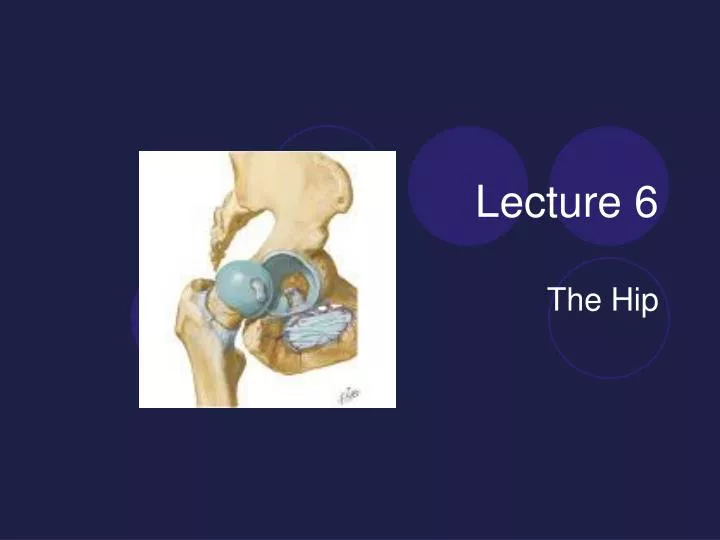
Lecture 6. The Hip. Anatomy Review Hip Joint Multi-axial ball and socket synovial joint It has maximum stability because of the deep socket (acetabulum)for the insertion of the head of the femur Strong ligaments and capsule encase this joint Acetabulum is deepened by a labrium.

E N D
Lecture 6 The Hip
Anatomy Review • Hip Joint • Multi-axial ball and socket synovial joint • It has maximum stability because of the deep socket (acetabulum)for the insertion of the head of the femur • Strong ligaments and capsule encase this joint • Acetabulum is deepened by a labrium
Hip Ligaments • Iliofemoral • Prevents excessive extension • Strongest in body • Ischiofemoral • Tight in extension • Pubofemoral • Prevents excessive abduction and extension • All three limit MR
Hip joint • Resting position 30 degrees flexion • 30 degrees abduction and • slight lateral rotation
Forces on the hip • Standing 0.3 X BW • Standing one leg 2.5 X BW • Walking 1.3-5.8 X BW • Upstairs 3 X BW • Running 4.5 X BW
Common problems • referred pain from back (lumbar spine) or SI to hip
Nerves • Majority of nerve supply arises from the Lumbar Plexus • Lumbar Plexus - formed from the first four lumbar spinal nerves • Largest branch is the Femoral nerve- supplies to the muscles and skin of the anterior thigh • Another branch Obturator nerve which provides innervation to the adductor muscles
Sacral plexus - L4 through S4 spinal nerves • Sciatic nerve arise from the sacral plexus • Sciatic innervate the hamstrings
Rom of Hip / End Feels • Flexion/ Extension • LR/MR • Abduction / Adduction • Muscles?
Thomas Test • Hip flexors • Hip flexion contracture • Athlete is supine with knees hanging over edge of table • Athlete brings knee up to chest , examiner can help push up so it is tight to chest • Positive test- if the hip flexor (iliopsoas) is tight on the opposite side the upper leg will lift up off the table
http://www.youtube.com/watch?v=wv4tYyRLXv8&feature=related • http://www.youtube.com/watch?v=RDBtb_IIf_U&feature=related
Rectus Femoris contracture ( Kendall Test) • Same as above – make sure they are right on edge of table • Now when they pull the knee to the chest look at the angle of the knee • If negative the knee should hang at 90 degrees • positive test - if the leg straightens out
Slump Test • Myofacial structures ( Dura) • Athlete is seated with both legs hanging over the edge of the table, tuck chin to chest and slump upper body forward • Examiner passively (or can be done actively by athlete) raises the leg to extension • Positive test- is pain ( limitations in Range) http://www.youtube.com/watch?v=GGGgospax-A&feature=related
Patrick FABER test • SI and General ROM of the hip • athlete Supine • foot on opposite knee • leg lowered in to abduction and LR • compare Left and right • positive test- is a difference in ROM and pain • http://www.youtube.com/watch?v=f_e-QqmBDJE
Tripod sign • Hamstring contracture • Athlete is seated with both legs hanging over the edge of the table • Examiner passively raises the leg to extension • Positive test - if the individual leans back to relieve the stress on the hamstrings
Trendelenburg sign • Weak Glut medius ( on stance side) • athlete standing on one leg must be able to stabilize hip • pelvis is level from left to right • Positive test - if ASIS ( pelvis) drops on non-stance side • Indicates a weakness or instability on stance side
Tests for leg length • The leg is anatomically or functionally shorter • Spine and pelvis (and others) will be affected due to kinetic chain • May lead to scoliosis, pelvic rotations and neck issues
Anatomical or True Leg length • To test measure from ASIS to medial malleolus (or lateral if muscle or fat get in way) heels approx 6 to 8 inches apart • Slight difference acceptable (1-1.3 cm considered normal) • If more than normal – measure tib and femur to see where difference is (can eyeball this • Side view and Front view
Functional or Apparent Leg Length • Results due to a compensation for a change that may have occurred because of positioning rather than structure • Unilateral pronation – spinal scoliosis, pelvic rotations • Can measure from umbilicus to medial malleolus • The test is only meaningful if the test for true leg length in negative
Muscle testing • Psoas and iliacus • Hip flexors • Athlete is seated with knees flexed • Hands on the edge of the table • Athlete lifts the upper leg off the table and examiner applies pressure on anterior surface of thigh downwards • Examiner stabilizes opposite side • Positive test – pain and weakness
Sartorious • Hip flexor, abductor and lateral rotator • Athlete is sitting or supine • Athlete brings ankle to opposite knee • Resistance applied to medial malleolus and to the lateral side of the thigh by examiner in an attempt to straighten the leg • Positive test – pain and weakness
Gluteus Maximus • Hip extension • Athlete is prone on table • Knee is flexed • Resistance is applied by examiner to the proximal knee (post thigh) in attempts to flex the hip • Stabilize above the hip (low back ) • Gluts work best when knee is flexed • Positive test – pain and weakness
Gluteus minimus and medius • As a hip abductor • Athlete is side lying with lower leg and hip flexed to 90 degrees • Resistance is applied to the proximal knee on the lateral side of the thigh • Movement should be without flexion or Lateral Rotator • Pelvis is stabilized • Positive test – pain and weakness
Gluteus minimus and medius • As a Medial Rotator • Athlete is supine or sitting • Knee flexed over the edge of table • Resistance is applied to the lateral malleolus pushing the leg medially • Positive test – pain and weakness
Adductors • Longus, magnus, brevis, gracillis and pectinus • Athlete is side lying • Non test limb is supported by the examiner • Lower limb is the test limb • Limb is adducted of the table and resistance is applied to the proximal knee joint medial thigh (pushing into abduction) • Positive test – pain and weakness
Lateral Rotators • Obturator Internus, Obturator Externus, Superior and Inferior Gemellies and Piriformis • Athlete is sitting with knee flexed over edge of table • Resistance is applied to the distal leg on the medial malleolus • Pushing lower leg laterally • Positive test – pain and weakness
Sport Specific Functional Tests • walking • going up and down stairs • running straight ahead , and variations • squatting • jumping